Furuichi Yumi, Kumamoto Kensuke, Asano Eisuke, Kondo Akihiro, Uemura Jun, Suto Hironobu, Oshima Minoru, Kishino Takayoshi, Usuki Hisashi, Okano Keiichi, Suzuki Yasuyuki
Department of Gastroenterological Surgery, Faculty of Medicine, Kagawa University, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa, 761-0793, Japan.
Surg Case Rep. 2020 Oct 2;6(1):255. doi: 10.1186/s40792-020-00988-6.
Persistent descending mesocolon (PDM) is a congenital anomaly associated with the failure of fixation of the descending colon to the lateral abdominal wall. In the laparoscopic colectomy for colorectal cancer, it has been noticed that there are extensive adhesions and a distinctive anatomy of colonic vessels in cases with PDM. Therefore, it is necessary to have sufficient knowledge about PDM so that it can be appropriately treated during surgery.
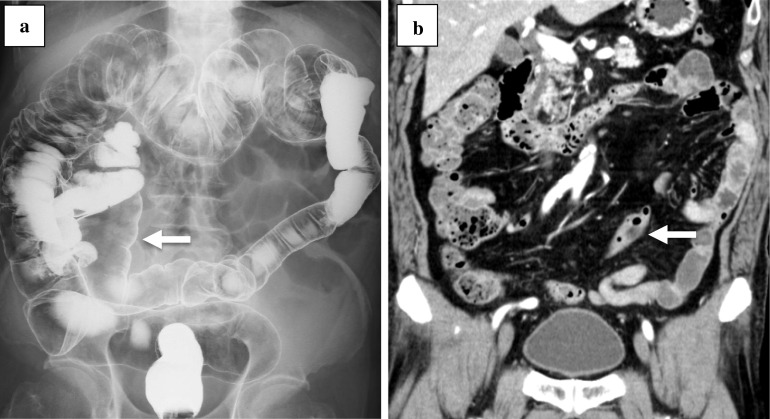
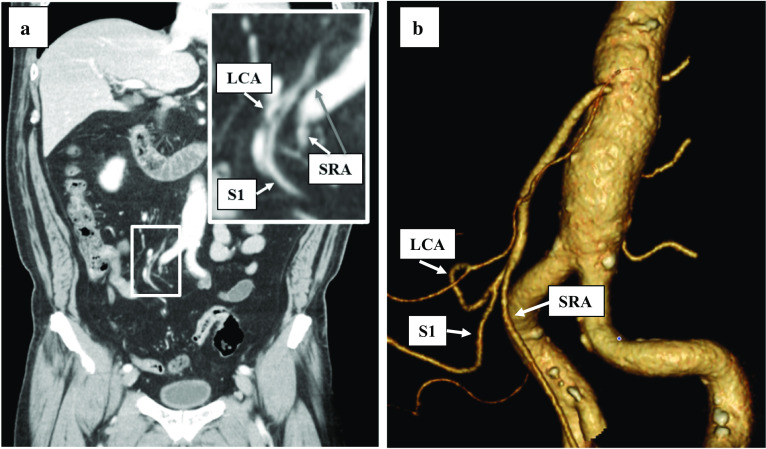
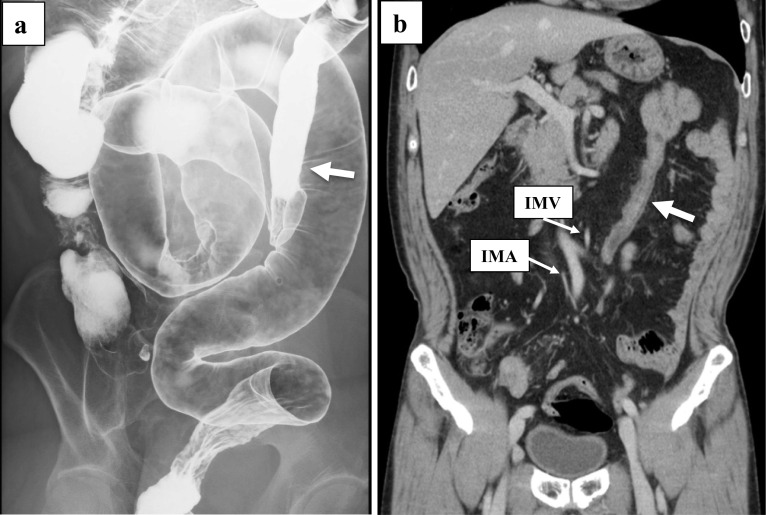
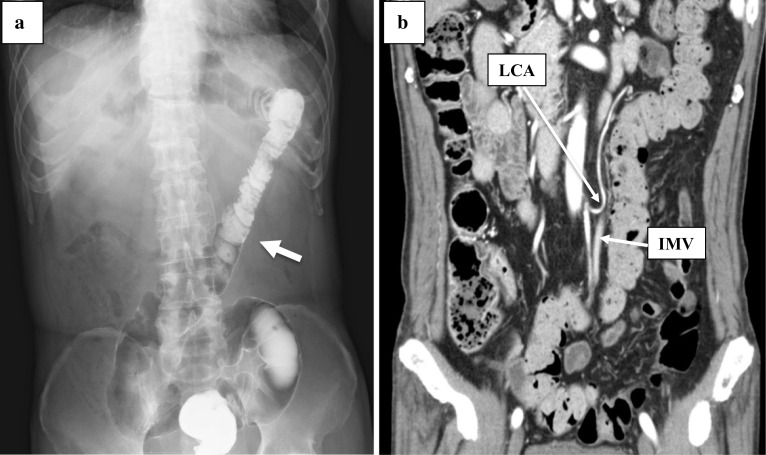
Case 1-a 79-year-old man underwent laparoscopic intersphincteric resection for rectal cancer. Preoperative barium enema (BE) revealed that the sigmoid colon was located at the right side of the abdomen. An enhanced computed tomography (CT) showed that the common trunk of the left colic artery (LCA) and the first sigmoid colonic artery (S1) branched from the inferior mesenteric artery (IMA). Case 2-a 68-year-old man underwent laparoscopic sigmoidectomy for sigmoid colon cancer and laparoscopic distal gastrectomy for gastric cancer synchronously. BE showed that the descending colon ran from the splenic flexure to medial caudal side. An enhanced CT showed that the distance from the LCA to the marginal artery was 1.0 cm. Case 3-a 68-year-old man underwent laparoscopic low anterior resection for rectal cancer. BE showed that the descending colon ran to the medial caudal side. An enhanced CT showed that the mesentery of the descending colon was comparatively shortened. Case 4-a 60-year-old man underwent laparoscopic sigmoidectomy for sigmoid colon cancer. An enhanced CT showed that the descending colon ran to the medial caudal side and predicted that the LCA and S1 formed a common trunk and branched radially from the IMA. We reported four cases with PDM recognized preoperatively as above. Three cases had a shortening of the mesocolon. While dissecting the vessels, although special attention was required to maintain the blood flow to the intestine, none of these cases developed any complications during the postoperative course.
We considered that it is important to have positional awareness of the LCA and the marginal artery to perform the laparoscopic surgery safely when a colorectal cancer with PDM is diagnosed preoperatively using imaging methods.
持续性降结肠系膜(PDM)是一种先天性异常,与降结肠固定于侧腹壁失败有关。在腹腔镜结直肠癌切除术中,已注意到PDM病例存在广泛粘连和结肠血管的独特解剖结构。因此,有必要对PDM有充分的了解,以便在手术中能对其进行适当处理。
病例1——一名79岁男性接受了直肠癌腹腔镜括约肌间切除术。术前钡剂灌肠(BE)显示乙状结肠位于腹部右侧。增强计算机断层扫描(CT)显示左结肠动脉(LCA)和第一乙状结肠动脉(S1)的共同干从肠系膜下动脉(IMA)分支。病例2——一名68岁男性同时接受了乙状结肠癌腹腔镜乙状结肠切除术和胃癌腹腔镜远端胃切除术。BE显示降结肠从脾曲向尾内侧走行。增强CT显示LCA至边缘动脉的距离为1.0厘米。病例3——一名68岁男性接受了直肠癌腹腔镜低位前切除术。BE显示降结肠向尾内侧走行。增强CT显示降结肠系膜相对缩短。病例4——一名60岁男性接受了乙状结肠癌腹腔镜乙状结肠切除术。增强CT显示降结肠向尾内侧走行,并预测LCA和S1形成共同干并从IMA呈放射状分支。我们报告了上述术前诊断为PDM的4例病例。3例存在结肠系膜缩短。在解剖血管时,尽管需要特别注意维持肠道血流,但这些病例在术后过程中均未出现任何并发症。
我们认为,当术前通过影像学方法诊断为伴有PDM的结直肠癌时,在进行腹腔镜手术时对LCA和边缘动脉有位置意识对于安全手术很重要。