Mansfield Carol A, Metcalfe Kelly A, Snyder Carrie, Lindeman Geoffrey J, Posner Joshua, Friedman Sue, Lynch Henry T, Narod Steven A, Evans D Gareth, Liede Alexander
RTI Health Solutions, Research Triangle Park, 3040 Cornwallis Road, PO Box 12194, Durham, NC 27709-12194 USA.
Women's College Hospital, University of Toronto, Toronto, Canada.
Hered Cancer Clin Pract. 2020 Sep 29;18:20. doi: 10.1186/s13053-020-00152-z. eCollection 2020.
Women with a or mutation have high lifetime risks of developing breast and ovarian cancer. The decision to embark on risk reduction strategies is a difficult and personal one. We surveyed an international group of women with mutations and measured choices and sequence of breast cancer risk reduction strategies.
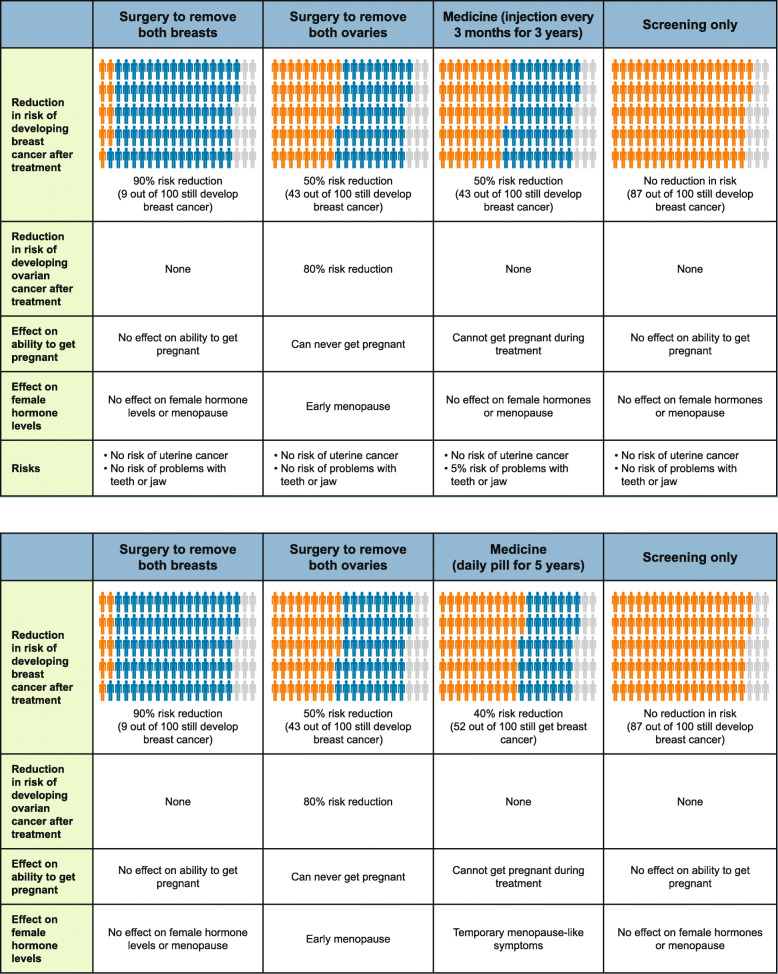
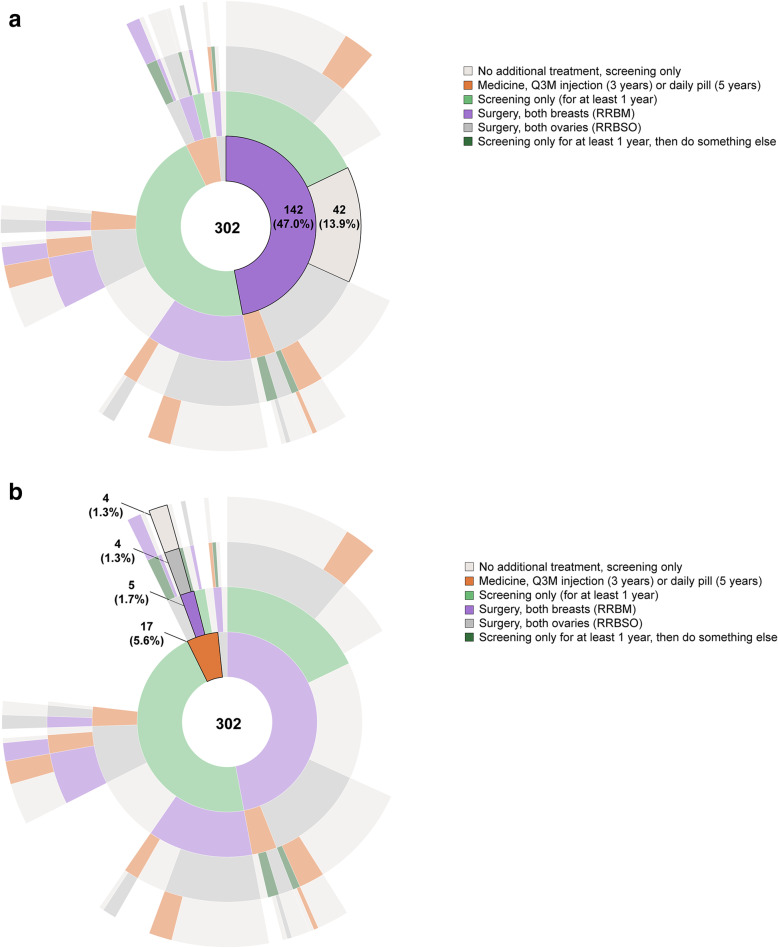
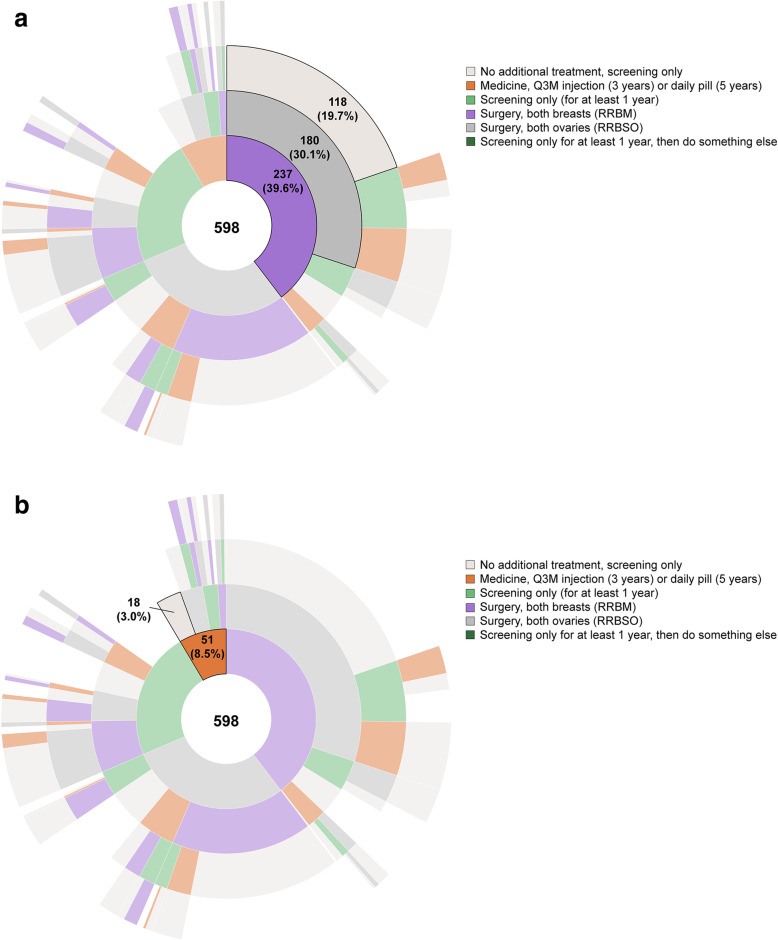
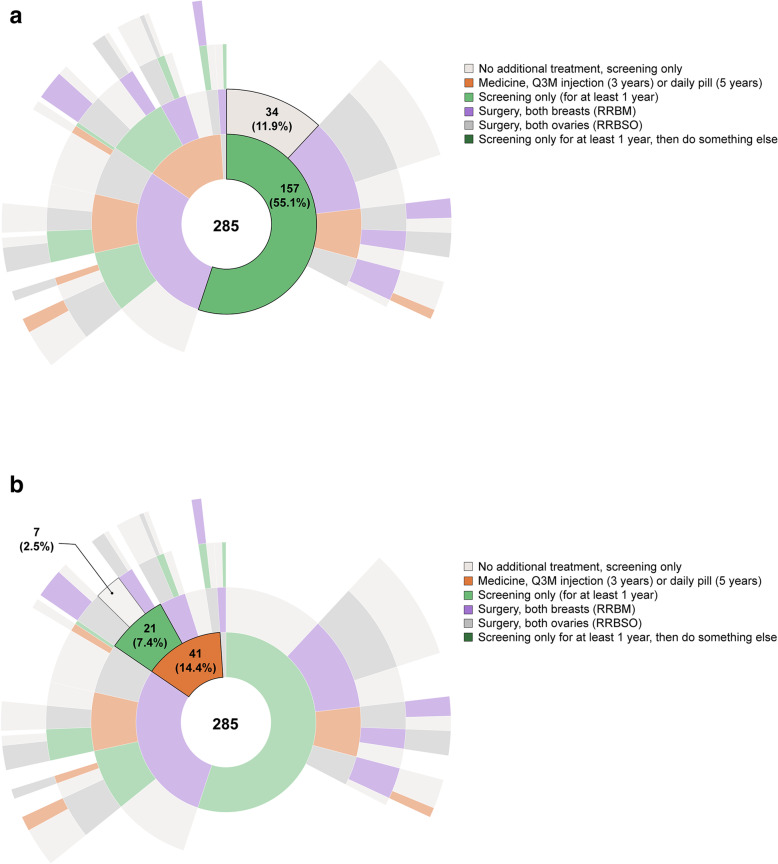
Women with a mutation and no previous cancer diagnosis were recruited from the US, Canada, the UK, Australia, and from a national advocacy group. Using an online survey, we asked about cancer-risk reduction preferences including for one of two hypothetical medicines, randomly assigned, and women's recommendations for a hypothetical woman (Susan, either a 25- or 36-year-old). Sunburst diagrams were generated to illustrate hierarchy of choices.
Among 598 respondents, mean age was 40.9 years (range 25-55 years). Timing of the survey was 4.8 years (mean) after learning their positive test result and 33% had risk-reducing bilateral salpingo-oophorectomy (RRBSO) and bilateral mastectomy (RRBM), while 19% had RRBSO only and 16% had RRBM only. Although 30% said they would take a hypothetical medicine, 6% reported taking a medicine resembling tamoxifen. Respondents were 1.5 times more likely to select a hypothetical medicine for risk reduction when Susan was 25 than when Susan was 36. Women assigned to 36-year-old Susan were more likely to choose a medicine if they had a family member diagnosed with breast cancer and personal experience taking tamoxifen.
Women revealed a willingness to undergo surgeries to achieve largest reduction in breast cancer risk, although this would not be recommended for a younger woman in her 20s. The goal of achieving the highest degree of cancer risk reduction is the primary driver for women with or mutations in selecting an intervention and a sequence of interventions, regardless of whether it is non-surgical or surgical.
携带BRCA1或BRCA2突变的女性一生中患乳腺癌和卵巢癌的风险很高。决定采取降低风险策略是一个艰难且因人而异的决定。我们对一组国际上携带BRCA突变的女性进行了调查,并评估了她们对降低乳腺癌风险策略的选择及顺序。
从美国、加拿大、英国、澳大利亚以及一个全国性倡导组织招募携带BRCA突变且此前未被诊断出患有癌症的女性。通过在线调查,我们询问了她们降低癌症风险的偏好,包括对两种随机分配的假设药物之一的偏好,以及她们对一位假设女性(25岁或36岁的苏珊)的建议。生成了旭日图以说明选择的层次结构。
在598名受访者中,平均年龄为40.9岁(范围25 - 55岁)。调查时间是在得知检测结果呈阳性后的4.8年(平均),33%的人进行了降低风险的双侧输卵管卵巢切除术(RRBSO)和双侧乳房切除术(RRBM),而19%的人仅进行了RRBSO,16%的人仅进行了RRBM。尽管30%的人表示愿意服用一种假设药物,但6%的人报告服用了类似他莫昔芬的药物。当苏珊为25岁时,受访者选择假设药物进行风险降低的可能性是苏珊为36岁时的1.5倍。如果分配给36岁的苏珊的受访者有家庭成员被诊断出患有乳腺癌且有服用他莫昔芬的个人经历,那么他们更有可能选择一种药物。
女性表示愿意接受手术以最大程度降低乳腺癌风险,尽管对于20多岁的年轻女性不建议这样做。实现最高程度的癌症风险降低这一目标是携带BRCA1或BRCA2突变的女性选择干预措施及干预顺序的主要驱动力,无论该干预措施是非手术的还是手术的。