Tjeertes Elke K M, van Fessem Joris M K, Mattace-Raso Francesco U S, Hoofwijk Anton G M, Stolker Robert Jan, Hoeks Sanne E
1Department of Anesthesiology, Erasmus MC University Medical Center, Rotterdam, the Netherlands.
2Department of Internal Medicine, Division of Geriatric Medicine, Erasmus MC University Medical Center, Rotterdam, the Netherlands.
Aging Dis. 2020 Oct 1;11(5):1276-1290. doi: 10.14336/AD.2019.1024. eCollection 2020 Oct.
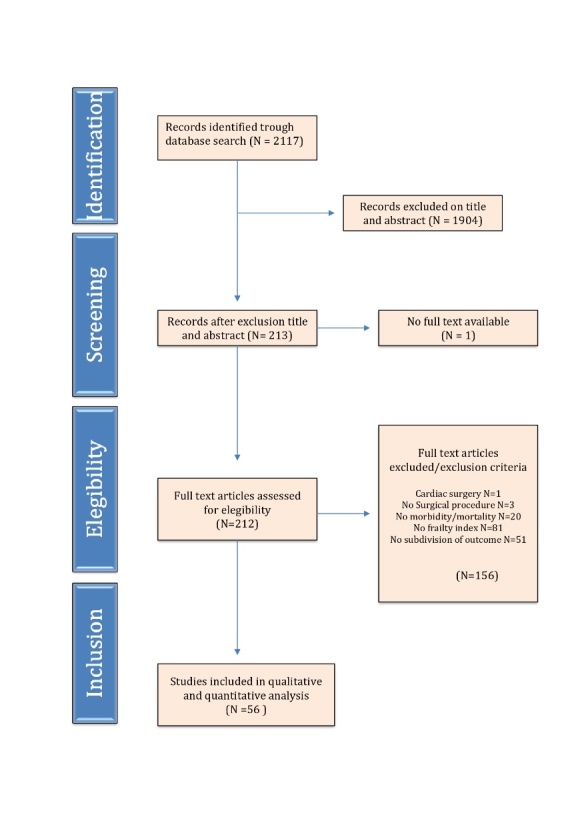
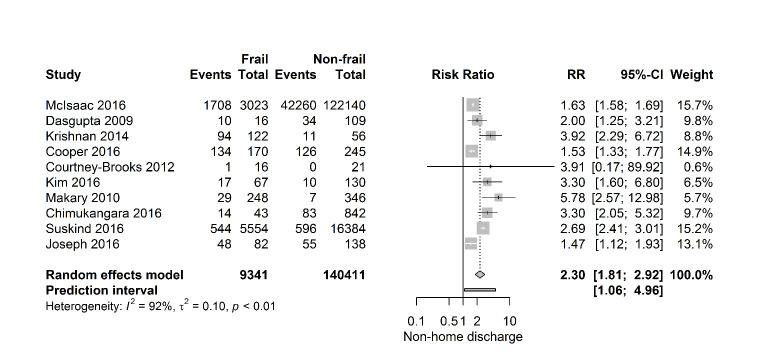
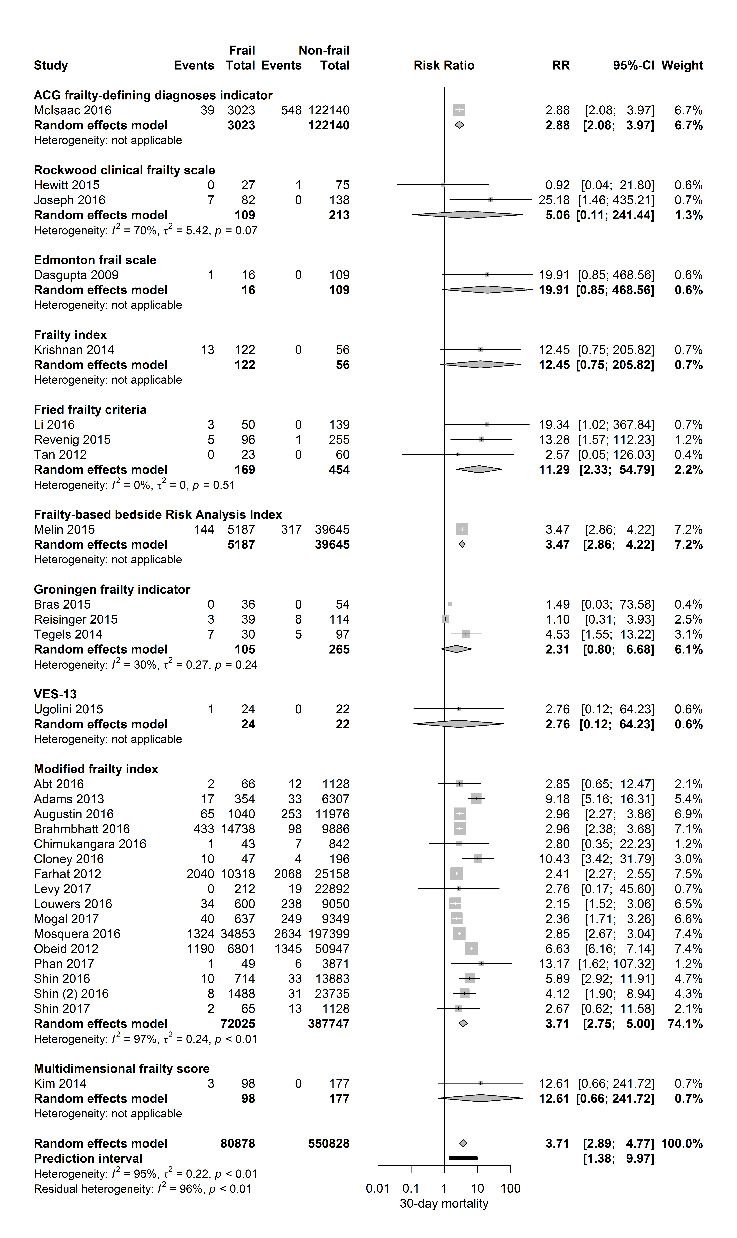
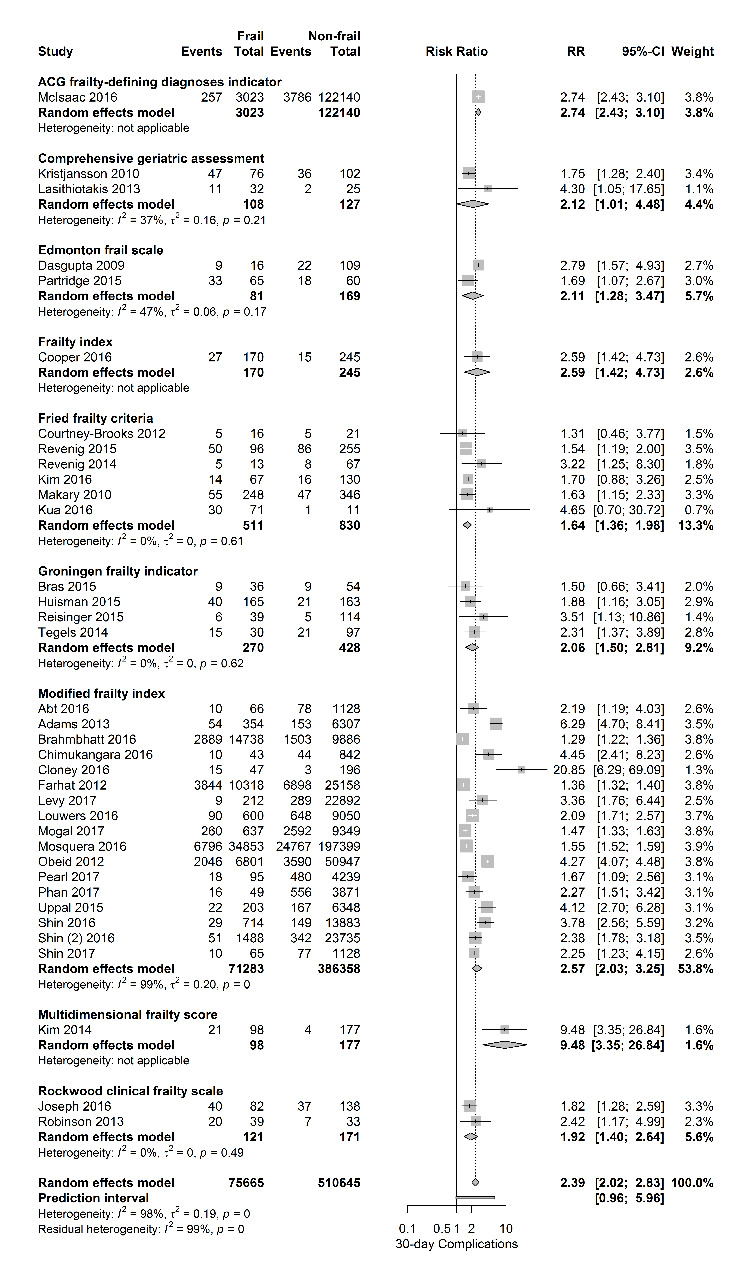
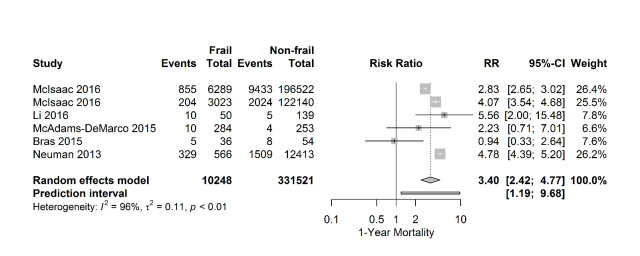
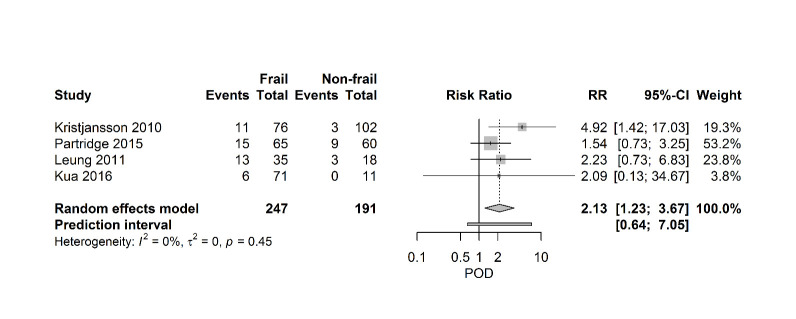
Frailty is increasingly recognized as a better predictor of adverse postoperative events than chronological age. The objective of this review was to systematically evaluate the effect of frailty on postoperative morbidity and mortality. Studies were included if patients underwent non-cardiac surgery and if frailty was measured by a validated instrument using physical, cognitive and functional domains. A systematic search was performed using EMBASE, MEDLINE, Web of Science, CENTRAL and PubMed from 1990 - 2017. Methodological quality was assessed using an assessment tool for prognosis studies. Outcomes were 30-day mortality and complications, one-year mortality, postoperative delirium and discharge location. Meta-analyses using random effect models were performed and presented as pooled risk ratios with confidence intervals and prediction intervals. We included 56 studies involving 1.106.653 patients. Eleven frailty assessment tools were used. Frailty increases risk of 30-day mortality (31 studies, 673.387 patients, risk ratio 3.71 [95% CI 2.89-4.77] (PI 1.38-9.97; I2=95%) and 30-day complications (37 studies, 627.991 patients, RR 2.39 [95% CI 2.02-2.83). Risk of 1-year mortality was threefold higher (six studies, 341.769 patients, RR 3.40 [95% CI 2.42-4.77]). Four studies (N=438) reported on postoperative delirium. Meta-analysis showed a significant increased risk (RR 2.13 [95% CI 1.23-3.67). Finally, frail patients had a higher risk of institutionalization (10 studies, RR 2.30 [95% CI 1.81- 2.92]). Frailty is strongly associated with risk of postoperative complications, delirium, institutionalization and mortality. Preoperative assessment of frailty can be used as a tool for patients and doctors to decide who benefits from surgery and who doesn't.
与实际年龄相比,虚弱越来越被认为是术后不良事件的更好预测指标。本综述的目的是系统评估虚弱对术后发病率和死亡率的影响。纳入的研究要求患者接受非心脏手术,且使用经过验证的工具通过身体、认知和功能领域来测量虚弱程度。使用EMBASE、MEDLINE、科学网、CENTRAL和PubMed对1990年至2017年的文献进行了系统检索。使用预后研究评估工具对方法学质量进行评估。结局指标为30天死亡率和并发症、1年死亡率、术后谵妄和出院地点。采用随机效应模型进行荟萃分析,并以合并风险比及置信区间和预测区间的形式呈现结果。我们纳入了56项研究,涉及1106653例患者。使用了11种虚弱评估工具。虚弱会增加30天死亡率的风险(31项研究,673387例患者,风险比3.71 [95%置信区间2.89 - 4.77](预测区间1.38 - 9.97;I² = 95%))和30天并发症的风险(37项研究,627991例患者,风险比2.39 [95%置信区间2.02 - 2.83])。1年死亡率的风险高出三倍(6项研究,341769例患者,风险比3.40 [95%置信区间2.42 - 4.77])。四项研究(N = 438)报告了术后谵妄情况。荟萃分析显示风险显著增加(风险比2.13 [95%置信区间1.23 - 3.67])。最后,虚弱患者入住机构的风险更高(10项研究,风险比2.30 [95%置信区间1.81 - 2.92])。虚弱与术后并发症、谵妄、入住机构和死亡风险密切相关。术前对虚弱的评估可作为患者和医生决定谁能从手术中获益以及谁不能获益的工具。