Departément de Medécine Nucléaire et Radiobiologie, Faculté de Medécine et des Sciences de la Santé, Université de Sherbrooke, Sherbrooke, QC J1H5N4, Canada.
Centre d'Imagerie Moleculaire, Centre de Rechcerche, Centre Hospitalier Universitaire de Sherbrooke (CHUS), Sherbrooke, QC J1H5N4, Canada.
Int J Mol Sci. 2020 Oct 1;21(19):7268. doi: 10.3390/ijms21197268.
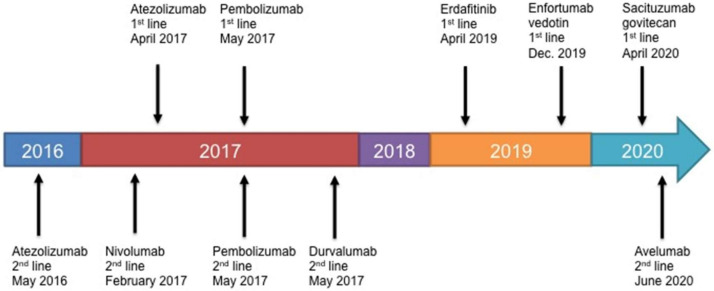
The fact that there are now five immune checkpoint inhibitor (ICI) monoclonal antibodies approved since 2016 that target programmed cell death protein 1 or programmed death ligand-1 for the treatment of metastatic and refractory bladder cancer is an outstanding achievement. Although patients can display pronounced responses that extend survival when treated with ICIs, the main benefit of these drugs compared to traditional chemotherapy is that they are better tolerated and result in reduced adverse events (AEs). Unfortunately, response rates to ICI treatment are relatively low and, these drugs are expensive and have a high economic burden. As a result, their clinical efficacy/cost-value relationship is debated. Long sought after targeted molecular therapeutics have now emerged and are boasting impressive response rates in heavily pre-treated, including ICI treated, patients with metastatic bladder cancer. The antibody-drug conjugates (ADCs) enfortumab vedotin (EV) and sacituzumab govitecan (SG) have demonstrated the ability to provide objective response rates (ORRs) of 44% and 31% in patients with bladder tumor cells that express Nectin-4 and Trop-2, respectively. As a result, EV was approved by the U.S. Food and Drug Administration for the treatment of patients with advanced or metastatic bladder cancer who have previously received ICI and platinum-containing chemotherapy. SG has been granted fast track designation. The small molecule Erdafitinib was recently approved for the treatment of patients with advanced or metastatic bladder cancer with genetic alterations in fibroblast growth factor receptors that have previously been treated with a platinum-containing chemotherapy. Erdafitinib achieved an ORR of 40% in patients including a proportion who had previously received ICI therapy. In addition, these targeted drugs are sufficiently tolerated or AEs can be appropriately managed. Hence, the early performance in clinical effectiveness of these targeted drugs are substantially increased relative to ICIs. In this article, the most up to date follow-ups on treatment efficacy and AEs of the ICIs and targeted therapeutics are described. In addition, drug price and cost-effectiveness are described. For best overall value taking into account clinical effectiveness, price and cost-effectiveness, results favor avelumab and atezolizumab for ICIs. Although therapeutically promising, it is too early to determine if the described targeted therapeutics provide the best overall value as cost-effectiveness analyses have yet to be performed and long-term follow-ups are needed. Nonetheless, with the arrival of targeted molecular therapeutics and their increased effectiveness relative to ICIs, creates a potential novel paradigm based on 'targeting' for affecting clinical practice for metastatic bladder cancer treatment.
自 2016 年以来,已有 5 种免疫检查点抑制剂(ICI)单克隆抗体被批准用于治疗转移性和难治性膀胱癌,这些药物靶向程序性细胞死亡蛋白 1 或程序性死亡配体 1,这是一项杰出的成就。尽管患者在接受 ICI 治疗时可以表现出明显的反应,从而延长生存期,但与传统化疗相比,这些药物的主要优势在于它们的耐受性更好,导致不良反应(AE)减少。不幸的是,ICI 治疗的反应率相对较低,而且这些药物昂贵,经济负担沉重。因此,它们的临床疗效/成本价值关系存在争议。人们长期以来一直寻求靶向分子疗法,现在已经出现了这些疗法,并在接受过大量预处理的转移性膀胱癌患者中,包括接受 ICI 治疗的患者中,显示出令人印象深刻的反应率。抗体药物偶联物(ADC)enfortumab vedotin(EV)和 sacituzumab govitecan(SG)分别在表达 Nectin-4 和 Trop-2 的膀胱肿瘤细胞患者中表现出 44%和 31%的客观缓解率(ORR)。因此,EV 被美国食品和药物管理局批准用于治疗先前接受过 ICI 和含铂化疗的晚期或转移性膀胱癌患者。SG 被授予快速通道指定。小分子 erdafitinib 最近被批准用于治疗先前接受过含铂化疗的晚期或转移性膀胱癌患者,这些患者具有成纤维细胞生长因子受体的遗传改变。erdafitinib 在包括先前接受过 ICI 治疗的患者在内的患者中实现了 40%的 ORR。此外,这些靶向药物具有足够的耐受性或可以适当管理不良反应。因此,与 ICI 相比,这些靶向药物在临床疗效方面的早期表现有了显著提高。在本文中,描述了 ICI 和靶向治疗的最新治疗疗效和不良反应随访结果。此外,还描述了药物价格和成本效益。为了获得最佳的总体价值,考虑到临床疗效、价格和成本效益,结果有利于avelumab 和 atezolizumab 作为 ICI。尽管具有治疗潜力,但要确定所描述的靶向治疗是否提供最佳的总体价值还为时过早,因为尚未进行成本效益分析,并且需要进行长期随访。尽管如此,随着靶向分子疗法的出现及其相对于 ICI 的有效性的提高,为转移性膀胱癌治疗的临床实践带来了一种基于“靶向”的潜在新范式。