Guan Jian, Jian Fengzeng, Yao Qingyu, Yuan Chenghua, Zhang Can, Ma Longbing, Liu Zhenlei, Duan Wanru, Wang Xingwen, Bo Xuefeng, Chen Zan
Division of Spine, Department of Neurosurgery, China International Neurological Institute, Xuanwu Hospital, Capital Medical University, Beijing, China.
School of Biomedical Engineering, Capital Medical University, Beijing, China.
Neurospine. 2020 Sep;17(3):574-584. doi: 10.14245/ns.2040496.248. Epub 2020 Sep 30.
This study evaluated the feasibility and efficacy of quantitative reduction and fixation to treat basilar invagination (BI) with atlantoaxial dislocation (AAD).
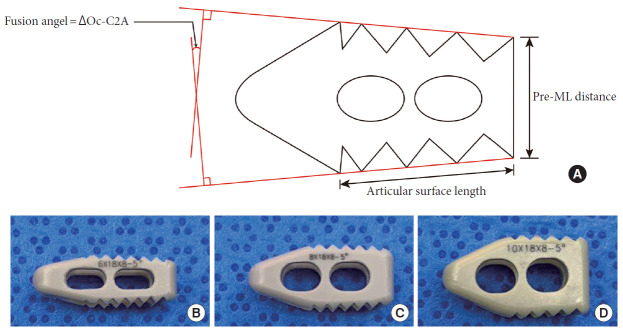
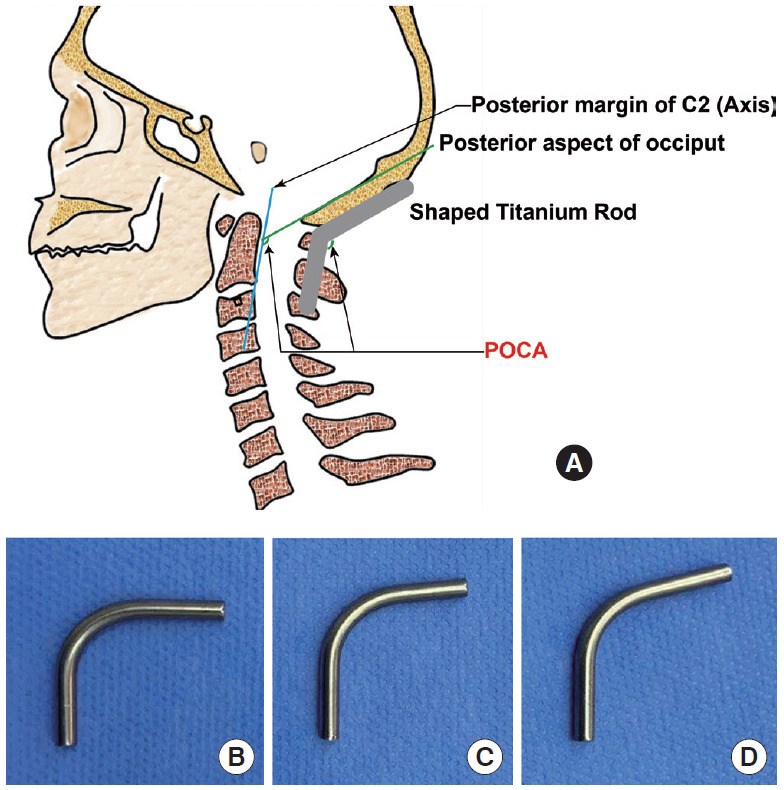
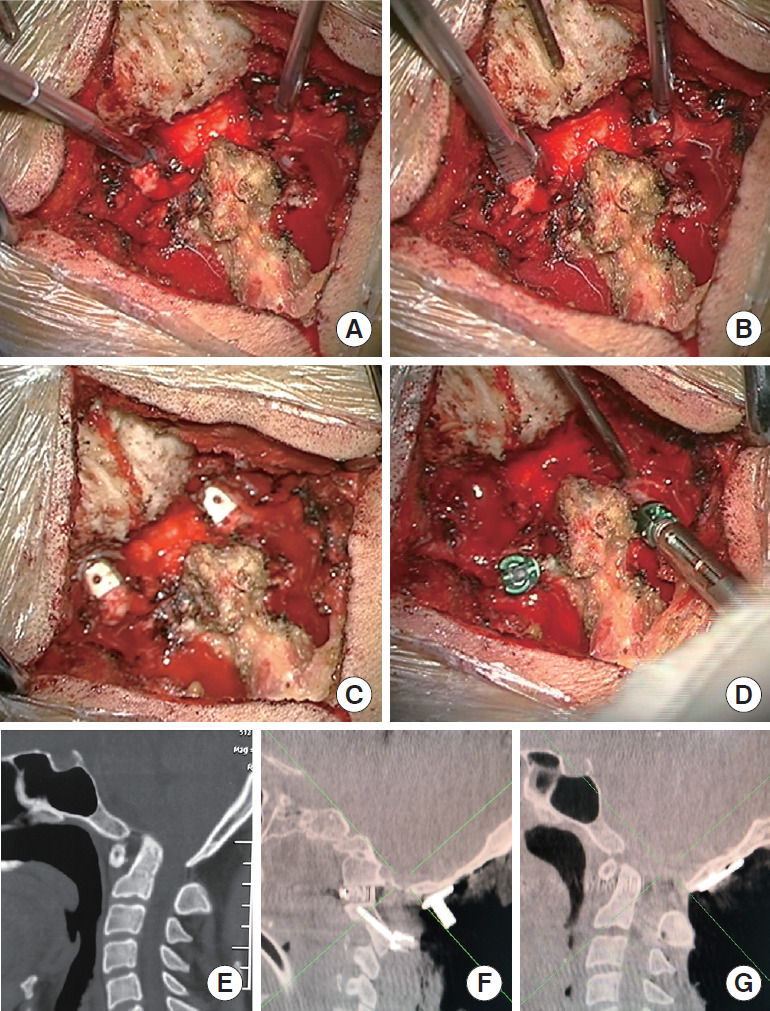
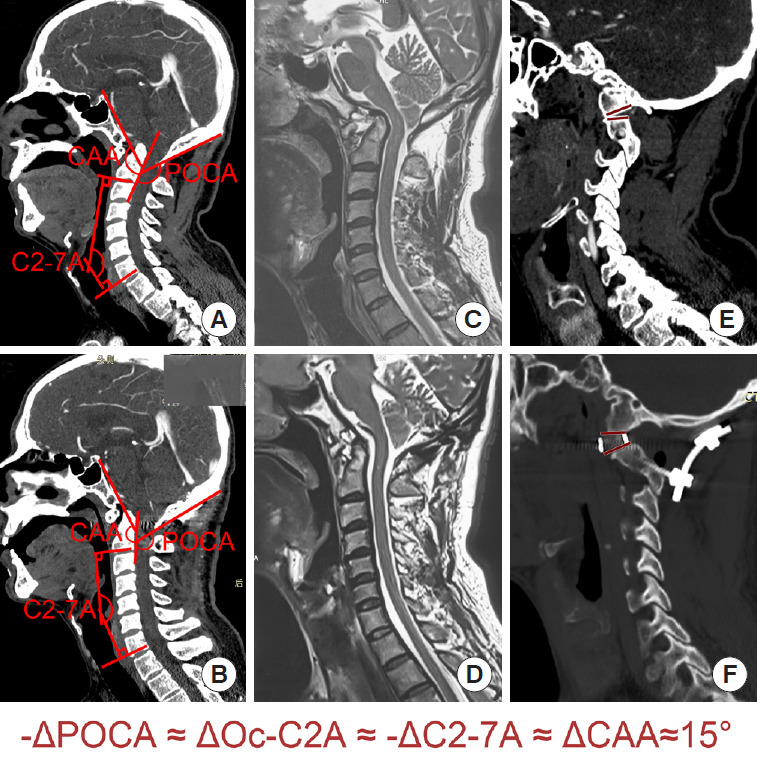
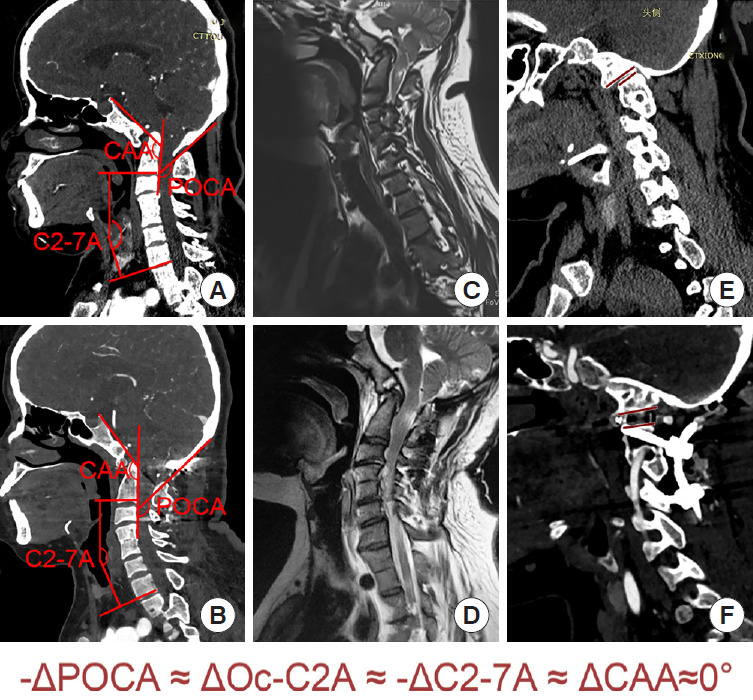
Posterior occipitocervical angle (POCA), occiput-C2 angle (Oc-C2A), clivusaxial angle (CAA), and C2-7 angle (C2-7A) were considered for quantitative reduction. Twelve patients with BI complicated with AAD received posterior interarticular release and individualized cage implantation to restore vertical dislocation. The POCA was adjusted using cantilever technology to further reduce the horizontal dislocation and adjust lower cervical vertebral angle. All patients received a radiological follow-up for ≥12 months. Improvements in spinal cord function were evaluated using Japanese Orthopedic Association (JOA) score.
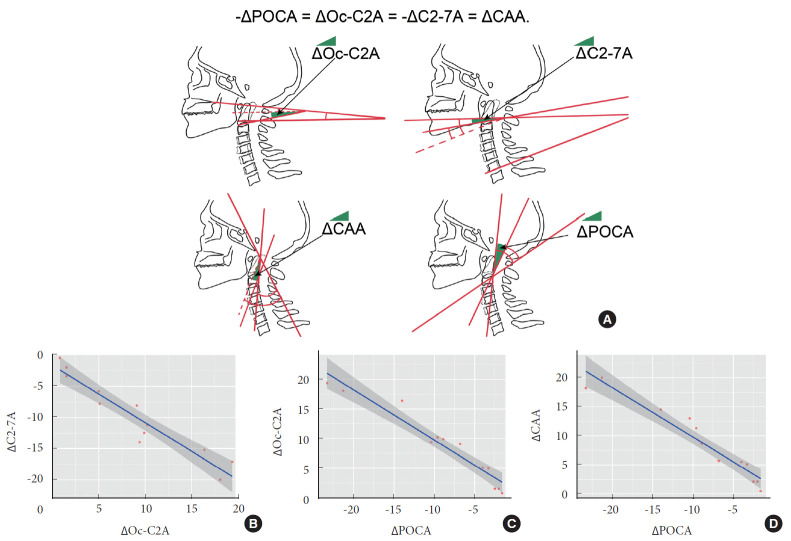
All the patients received successful quantitative reduction for BI-AAD, and bony fusion was achieved without spinal cord injury after surgery for 12 months. The JOA score was improved significantly to 15.2 ± 0.9 twelve months after surgery (p < 0.01). Radiological follow-up revealed that individualized cage and POCA play vital roles in quantitative correction: (1) distance of the dens above McRae's line and atlantodens interval were restored to normal level, respectively; (2) changes in Oc-C2 angle (ΔOc-C2A), C2-7 angle (ΔC2-7A), clivus-axial angle (ΔCAA), and POCA (ΔPOCA) were all caused by changes in axis tilt. Based on the changes of radiological parameter we deduced the formula for quantitative reduction by linear regression analysis: -ΔPOCA = ΔOc-C2A = -ΔC2-7A = ΔCAA.
Quantitative posterior reduction by individualized cage and adjusting ΔPOCA is feasible for treating BI with AAD.
本研究评估定量复位与固定治疗合并寰枢椎脱位(AAD)的基底凹陷症(BI)的可行性和疗效。
采用后枕颈角(POCA)、枕骨 - C2角(Oc - C2A)、斜坡 - 枢椎角(CAA)和C2 - 7角(C2 - 7A)进行定量复位。12例合并AAD的BI患者接受了后关节间松解和个体化椎间融合器植入以恢复垂直脱位。使用悬臂技术调整POCA以进一步减少水平脱位并调整下颈椎角度。所有患者均接受了≥12个月的影像学随访。采用日本骨科学会(JOA)评分评估脊髓功能改善情况。
所有患者的BI - AAD均成功进行了定量复位,术后12个月实现了骨融合且无脊髓损伤。术后12个月JOA评分显著提高至15.2±0.9(p < 0.01)。影像学随访显示,个体化椎间融合器和POCA在定量矫正中起关键作用:(1)齿状突高于McRae线的距离和寰齿间隙分别恢复至正常水平;(2)Oc - C2角(ΔOc - C2A)、C2 - 7角(ΔC2 - 7A)、斜坡 - 枢椎角(ΔCAA)和POCA(ΔPOCA)的变化均由枢椎倾斜度的改变引起。基于影像学参数的变化,我们通过线性回归分析推导了定量复位公式:-ΔPOCA = ΔOc - C2A = -ΔC2 - 7A = ΔCAA。
采用个体化椎间融合器和调整ΔPOCA进行后路定量复位治疗合并AAD的BI是可行的。