Kaiser Permanente South Sacramento Medical Center, Sacramento, CA.
Division of Research, Kaiser Permanente Northern California, CA.
J Am Coll Surg. 2021 Jan;232(1):35-44. doi: 10.1016/j.jamcollsurg.2020.09.015. Epub 2020 Oct 3.
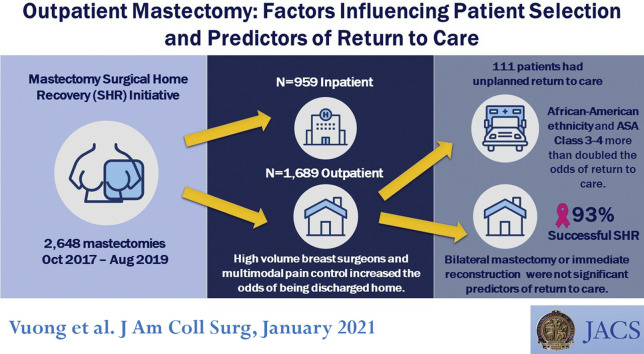
After implementation of the Surgical Home Recovery (SHR) initiative for mastectomy within a large, integrated health delivery system, most patients are discharged on the day of the procedure. We sought to identify predictors of SHR and unplanned return to care (RTC).
Mastectomy cases with and without reconstruction from October 2017 to August 2019 were analyzed. Patient characteristics, operative variables, and multimodal pain management were compared between admitted patients and SHR patients using logistic regression. We identified predictors of RTC in SHR patients, defined as 7-day readmission, reoperation, or emergency department visit.
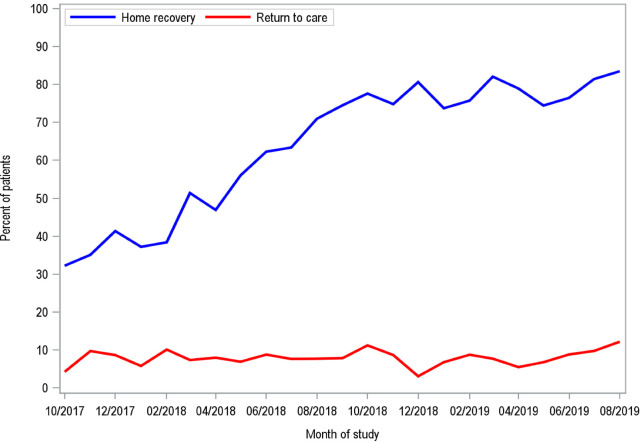
Of 2,648 mastectomies, 1,689 (64%) were outpatient procedures and the mean age of patients was 58.5 years. Predictors of SHR included perioperative IV acetaminophen (odds ratio [OR] 1.59; 95% CI, 1.28 to 1.97), perioperative opiates (OR 1.47; 95% CI, 1.06 to 2.02), and operation performed by a high-volume breast surgeon (OR 2.12; 95% CI, 1.42 to 3.18). Bilateral mastectomies (OR 0.70; 95% CI, 0.54 to 0.91), immediate reconstruction (OR 0.52; 95% CI, 0.39 to 0.70), and American Society of Anesthesiologists class 3 to 4 (OR 0.69; 95% CI, 0.54 to 0.87) decreased the odds of SHR. Of SHR patients, 111 of 1,689 patients (7%) experienced RTC. Patients with American Society of Anesthesiologists class 3 to 4 (OR 2.01; 95% CI, 1.29 to 3.14) and African American race (OR 2.30; 95% CI, 1.38 to 4.91) were more likely to RTC; receiving IV acetaminophen (OR 0.56; 95% CI, 0.35 to 0.88) and filling an opiate prescription (OR 0.51; 95% CI, 0.34 to 0.77) decreased the odds of RTC.
Surgeon volume and multimodal pain medication increased the odds of SHR. Within the SHR group, American Society of Anesthesiologists Class 3 to 4 and African American patients increased the likelihood of RTC. This study helps optimize patient selection and perioperative practice for successful SHR.
在大型综合医疗服务系统中实施乳房切除术的“手术之家康复(SHR)”计划后,大多数患者在手术当天出院。我们试图确定 SHR 和计划外返院(RTC)的预测因素。
对 2017 年 10 月至 2019 年 8 月期间有和无重建的乳房切除术病例进行分析。使用逻辑回归比较住院患者和 SHR 患者的患者特征、手术变量和多模式疼痛管理。我们确定了 SHR 患者 RTC 的预测因素,定义为 7 天内再入院、再次手术或急诊就诊。
在 2648 例乳房切除术中,1689 例(64%)为门诊手术,患者平均年龄为 58.5 岁。SHR 的预测因素包括围手术期 IV 扑热息痛(优势比 [OR] 1.59;95%CI,1.28 至 1.97)、围手术期阿片类药物(OR 1.47;95%CI,1.06 至 2.02)和高容量乳房外科医生进行的手术(OR 2.12;95%CI,1.42 至 3.18)。双侧乳房切除术(OR 0.70;95%CI,0.54 至 0.91)、即刻重建(OR 0.52;95%CI,0.39 至 0.70)和美国麻醉师协会(ASA)分级 3 至 4 级(OR 0.69;95%CI,0.54 至 0.87)降低了 SHR 的可能性。在 SHR 患者中,1689 例患者中有 111 例(7%)经历了 RTC。ASA 分级 3 至 4 级(OR 2.01;95%CI,1.29 至 3.14)和非裔美国人(OR 2.30;95%CI,1.38 至 4.91)的患者更有可能 RTC;接受 IV 扑热息痛(OR 0.56;95%CI,0.35 至 0.88)和开具阿片类药物处方(OR 0.51;95%CI,0.34 至 0.77)降低了 RTC 的可能性。
外科医生的手术量和多模式疼痛药物增加了 SHR 的可能性。在 SHR 组中,ASA 分级 3 至 4 级和非裔美国人患者增加了 RTC 的可能性。这项研究有助于优化患者选择和围手术期实践,以实现成功的 SHR。