Division of Cardiology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand.
Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand.
BMC Cardiovasc Disord. 2020 Oct 6;20(1):433. doi: 10.1186/s12872-020-01716-6.
Significant tricuspid regurgitation (TR) can be found in patients with atrial fibrillation (AF). The results of previous studies are controversial about whether significant functional TR (FTR) in patients with AF leads to worse clinical outcomes. The aims of the study were to investigate the prevalence, predictors and prognosis of significant FTR in patients with AF with preserved left ventricular ejection fraction (LVEF).
The present study was a retrospective cohort study in patients with AF and preserved LVEF from May 2013 through January 2018. Significant FTR was defined as moderate to severe TR without structural abnormality of the tricuspid valve. Pulmonary hypertension (PH) was defined as pulmonary artery systolic pressure ≥ 50 mmHg or mean pulmonary artery pressure ≥ 25 mmHg determined by echocardiography. The adverse outcomes were defined as heart failure and death from any cause within 2 years of follow up.
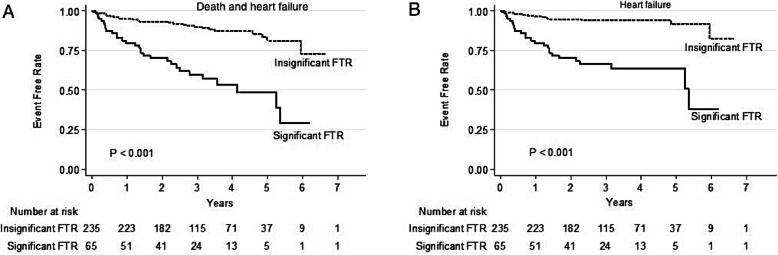
A total of 300 patients with AF (mean age 68.8 ± 10.8 years, 50% male) were included in the study. Paroxysmal and non-paroxysmal AF were reported in 34.7 and 65.3% of patients, respectively. Mean LVEF was 65.3 ± 6.3%. PH and significant FTR were observed in 31.3 and 21.7% of patients, respectively. Patients with significant FTR were significantly older, more female gender and non-paroxysmal AF, and had higher left atrial volume index and pulmonary artery pressure than those without. A total of 26 (8.7%) patients died and heart failure occurred in 39 (13.0%) patients. There was a statistically significant difference in the adverse outcomes between patients with significant and insignificant FTR (44.6% vs. 11.9%, p < 0.010). Multivariable analysis showed that factors associated with significant FTR were female gender, presence of PH and left atrial volume index (OR = 2.61, 1.87, and 1.04, respectively). The predictors of the adverse outcomes in patients with AF were significant FTR, presence of PH and high CHADS-VASc score (OR = 5.23, 2.23 and 1.60, respectively).
Significant FTR was common in patients with AF, and independently associated with adverse outcomes. Thus, comprehensive echocardiographic assessment of FTR in patients with AF and preserved LVEF is fundamental in determining the optimal management.
在心房颤动(AF)患者中可发现明显的三尖瓣反流(TR)。关于 AF 患者是否存在明显的功能性三尖瓣反流(FTR)会导致更差的临床结局,之前的研究结果存在争议。本研究的目的是调查射血分数保留的 AF 患者中存在明显 FTR 的患病率、预测因素和预后。
本研究是 2013 年 5 月至 2018 年 1 月期间射血分数保留的 AF 患者的回顾性队列研究。明显的 FTR 定义为无三尖瓣结构异常的中度至重度 TR。肺动脉高压(PH)定义为通过超声心动图确定的肺动脉收缩压≥50mmHg 或平均肺动脉压≥25mmHg。不良结局定义为在 2 年随访期间心力衰竭和任何原因导致的死亡。
共纳入 300 例 AF 患者(平均年龄 68.8±10.8 岁,50%为男性)。阵发性和非阵发性 AF 分别占 34.7%和 65.3%。平均 LVEF 为 65.3±6.3%。31.3%和 21.7%的患者分别存在 PH 和明显的 FTR。与无明显 FTR 的患者相比,有明显 FTR 的患者年龄更大,女性更多,非阵发性 AF 更多,左心房容积指数和肺动脉压更高。共有 26 例(8.7%)患者死亡,39 例(13.0%)患者发生心力衰竭。有明显和无明显 FTR 的患者不良结局的发生率有统计学差异(44.6%比 11.9%,p<0.010)。多变量分析显示,与明显 FTR 相关的因素是女性、存在 PH 和左心房容积指数(OR=2.61、1.87 和 1.04)。AF 患者不良结局的预测因素是明显的 FTR、存在 PH 和高 CHADS-VASc 评分(OR=5.23、2.23 和 1.60)。
在 AF 患者中,明显的 FTR 很常见,与不良结局独立相关。因此,对射血分数保留的 AF 患者进行全面的 FTR 超声心动图评估对于确定最佳治疗方案至关重要。