Department of Cardiology, Leiden University Medical Center, Leiden, The Netherlands.
Department of Surgery, Leiden University Medical Center, Leiden, The Netherlands.
Sci Rep. 2020 Oct 6;10(1):16601. doi: 10.1038/s41598-020-73608-w.
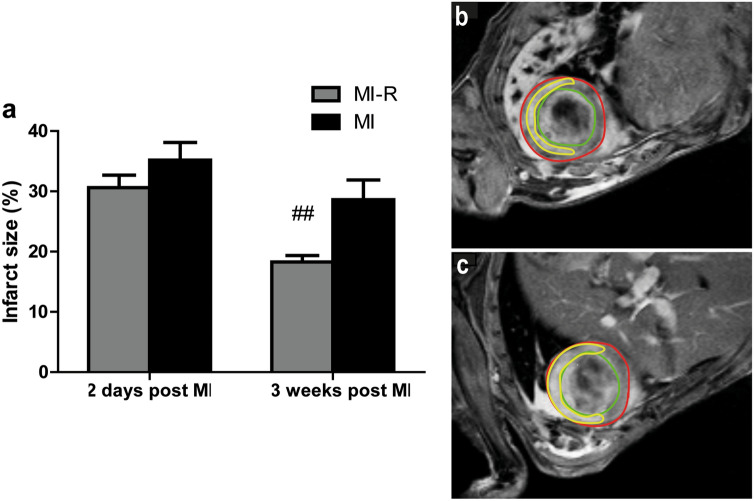
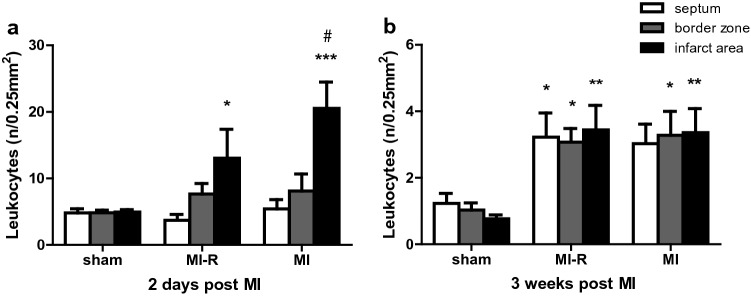
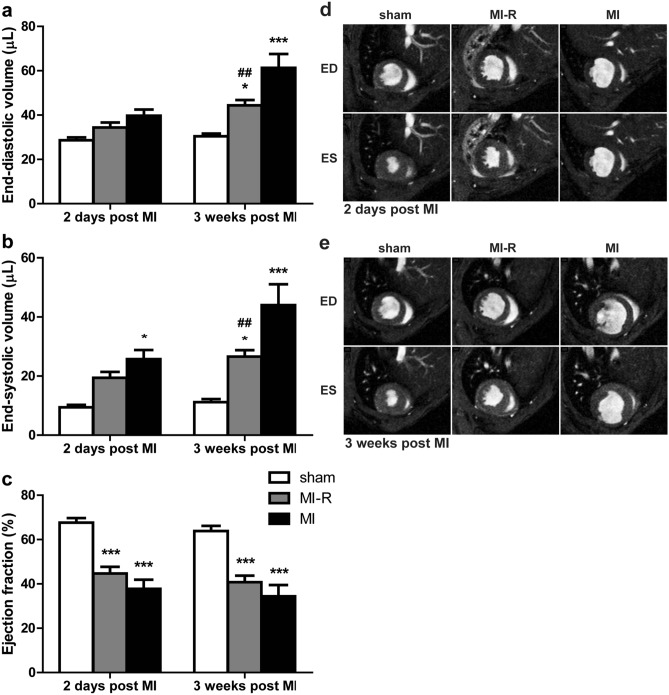
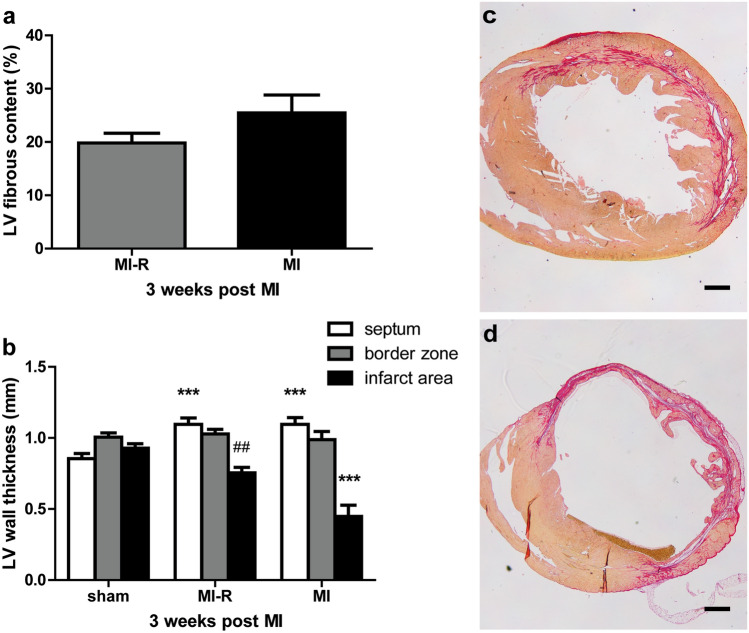
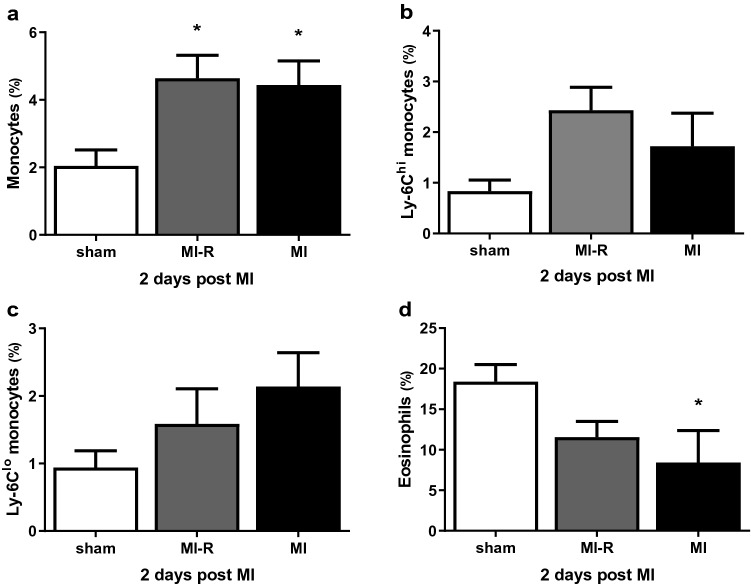
Many novel therapies to treat myocardial infarction (MI), yielding promising results in animal models, nowadays failed in clinical trials for several reasons. The most used animal MI model is based on permanent ligation of the left anterior descending (LAD) coronary artery in healthy mice resulting in transmural MI, while in clinical practice reperfusion is usually accomplished by primary percutaneous coronary interventions (PCI) limiting myocardial damage and inducing myocardial ischemia-reperfusion (MI-R) injury. To evaluate a more similar murine MI model we compared MI-R injury to unreperfused MI in hypercholesterolemic apolipoprotein (APO)E*3-Leiden mice regarding effects on cardiac function, left ventricular (LV) remodeling and inflammation. Both MI-R and MI resulted in significant LV dilation and impaired cardiac function after 3 weeks. Although LV dilation, displayed by end-diastolic (EDV) and end-systolic volumes (ESV), and infarct size (IS) were restricted following MI-R compared to MI (respectively by 27.6% for EDV, 39.5% ESV, 36.0% IS), cardiac function was not preserved. LV-wall thinning was limited with non-transmural LV fibrosis in the MI-R group (66.7%). Two days after inducing myocardial ischemia, local leucocyte infiltration in the infarct area was decreased following MI-R compared to MI (36.6%), whereas systemic circulating monocytes were increased in both groups compared to sham (130.0% following MI-R and 120.0% after MI). Both MI-R and MI models against the background of a hypercholesterolemic phenotype appear validated experimental models, however reduced infarct size, restricted LV remodeling as well as a different distributed inflammatory response following MI-R resemble the contemporary clinical outcome regarding primary PCI more accurately which potentially provides better predictive value of experimental therapies in successive clinical trials.
许多治疗心肌梗死 (MI) 的新型疗法在动物模型中取得了有前景的结果,但由于多种原因,在临床试验中失败了。最常用的动物 MI 模型是基于健康小鼠左前降支 (LAD) 冠状动脉的永久性结扎,导致透壁 MI,而在临床实践中,再灌注通常通过经皮冠状动脉介入治疗 (PCI) 来实现,限制了心肌损伤并诱导心肌缺血再灌注 (MI-R) 损伤。为了评估一种更相似的小鼠 MI 模型,我们比较了高脂血症载脂蛋白 (APO)E*3-Leiden 小鼠的 MI-R 损伤与未再灌注 MI,以评估对心脏功能、左心室 (LV) 重构和炎症的影响。MI-R 和 MI 均导致 3 周后 LV 扩张和心脏功能受损。尽管与 MI 相比,MI-R 后 LV 扩张(通过舒张末期 (EDV) 和收缩末期容积 (ESV) 显示)和梗死面积 (IS) 受到限制(分别为 EDV 减少 27.6%,ESV 减少 39.5%,IS 减少 36.0%),但心脏功能并未得到保留。MI-R 组 LV 壁变薄,伴有非透壁 LV 纤维化(66.7%)。MI-R 后 2 天,与 MI 相比,梗死区局部白细胞浸润减少(36.6%),而两组循环单核细胞均高于假手术组(MI-R 后为 130.0%,MI 后为 120.0%)。在高脂血症表型的背景下,MI-R 和 MI 模型均为有效的实验模型,然而,MI-R 后梗死面积减小、LV 重构受限以及不同分布的炎症反应更类似于当代临床结果,更准确地反映了经皮冠状动脉介入治疗的结果,从而为后续临床试验中的实验治疗提供了更好的预测价值。