Shiau Henry, Guffey Danielle, Loomes Kathleen M, Seidman Christa, Ragozzino Emily, Molleston Jean P, Schady Deborah, Leung Daniel H
Pediatric Gastroenterology, Hepatology, and Nutrition Baylor College of Medicine Houston TX.
Texas Children's Hospital Houston TX.
Hepatol Commun. 2020 Aug 1;4(10):1516-1526. doi: 10.1002/hep4.1569. eCollection 2020 Oct.
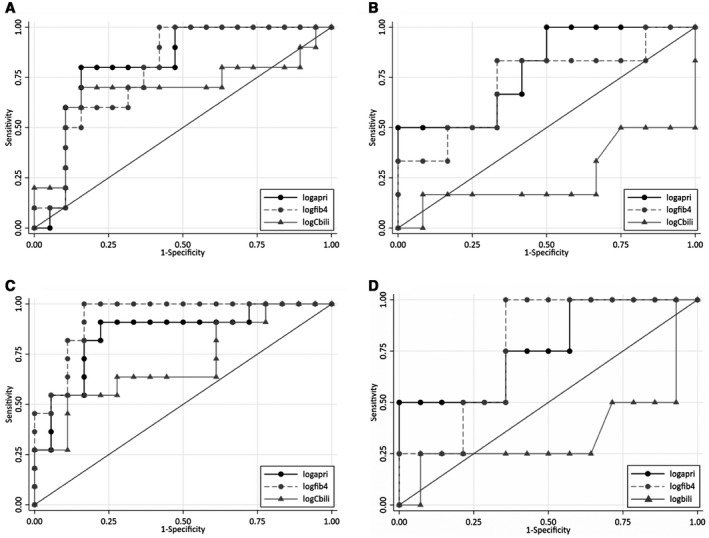
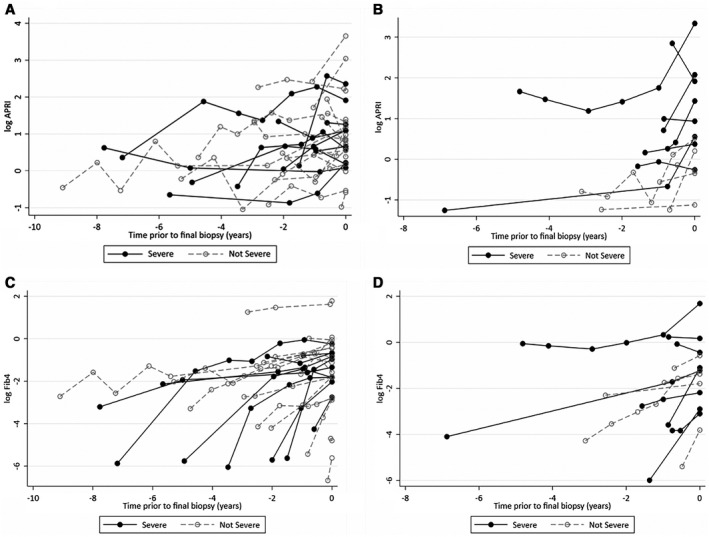
Alagille syndrome (ALGS) and progressive familial intrahepatic cholestasis (PFIC) are inherited cholestatic disorders with risk of developing end-stage liver disease requiring liver transplantation (LT). We investigated aspartate aminotransferase-to-platelet ratio index (APRI), Fibrosis-4 score (FIB-4), and conjugated bilirubin as biomarkers to assess fibrosis severity and risk for LT among children with ALGS and PFIC. This multicenter, cross-sectional study included 64 children with ALGS or PFIC (per genetics or strict clinical criteria) with APRI, FIB-4, and conjugated bilirubin levels collected within ±90 days of their most recent liver biopsy. A single, blinded pathologist staged all biopsies (metavir; F0-F2: nonsevere, F3-F4: severe). Logistic regression and area under the receiver operating characteristic curve analysis (AUC) were used to assess biomarker associations with fibrosis severity and risk for LT. In ALGS, only APRI distinguished F3-F4 (AUC 0.72, = 0.012), with a cutoff greater than 2.97 demonstrating a sensitivity of 61.5% (95% confidence interval 0.32, 0.86) and specificity of 81.5% (0.62, 0.94). In ALGS, a 50% increase of APRI increased the odds of F3-F4 by 1.31-fold (1.04, 1.65; = 0.023). In ALGS, APRI (AUC 0.87; < 0.001) and FIB-4 (AUC 0.84; < 0.001) were able to predict risk for LT. In PFIC, only APRI distinguished F3-4 (AUC 0.74, = 0.039), with a cutoff greater than 0.99 demonstrating a sensitivity of 80% (0.44, 0.98) and specificity of 64.3% (0.35, 0.87). In PFIC, only FIB-4 was able predict risk for LT (AUC 0.80; = 0.002). In ALGS or PFIC, conjugated bilirubin could not distinguish F3-F4 or predict risk for LT. This liver biopsy-validated study suggests that APRI is able to distinguish F3-F4 from F0-F2 in ALGS and PFIC. APRI and FIB-4 may also serve as predictors of risk for LT in ALGS (APRI and FIB-4) and PFIC (FIB-4).
阿拉吉尔综合征(ALGS)和进行性家族性肝内胆汁淤积症(PFIC)是遗传性胆汁淤积性疾病,有发展为需要肝移植(LT)的终末期肝病的风险。我们研究了天冬氨酸转氨酶与血小板比值指数(APRI)、纤维化-4评分(FIB-4)和结合胆红素作为生物标志物,以评估ALGS和PFIC患儿的纤维化严重程度和肝移植风险。这项多中心横断面研究纳入了64例ALGS或PFIC患儿(根据遗传学或严格的临床标准),在其最近一次肝活检的±90天内收集了APRI、FIB-4和结合胆红素水平。由一名单盲病理学家对所有活检进行分期(梅塔维分级;F0-F2:非重度,F3-F4:重度)。采用逻辑回归和受试者操作特征曲线下面积分析(AUC)来评估生物标志物与纤维化严重程度和肝移植风险的相关性。在ALGS中,只有APRI能够区分F3-F4(AUC 0.72,P = 0.012),临界值大于2.97时,敏感性为61.5%(95%置信区间0.32,0.86),特异性为B1.5%(0.62,0.94)。在ALGS中,APRI增加50%会使F3-F4的几率增加1.31倍(1.04,1.65;P = 0.023)。在ALGS中,APRI(AUC 0.87;P < 0.001)和FIB-4(AUC 0.84;P < 0.001)能够预测肝移植风险。在PFIC中,只有APRI能够区分F3-4(AUC 0.74,P = 0.039),临界值大于0.99时,敏感性为80%(0.44,0.98),特异性为64.3%(0.35,0.B7)。在PFIC中,只有FIB-4能够预测肝移植风险(AUC 0.80;P = 0.002)。在ALGS或PFIC中,结合胆红素无法区分F3-F4或预测肝移植风险。这项经肝活检验证的研究表明,APRI能够在ALGS和PFIC中区分F3-F4与F0-F2。APRI和FIB-4也可能作为ALGS(APRI和FIB-4)和PFIC(FIB-4)肝移植风险的预测指标。