University of Illinois at Urbana-Champaign, 1406 W. Green St, Urbana, IL, 61801, USA.
Korea Polytechnic University, 237 Sangidaehak-ro, Siheung-si, Gyeonggi-do, 15073, South Korea.
BMC Med Inform Decis Mak. 2020 Oct 7;20(1):255. doi: 10.1186/s12911-020-01262-3.
Clinical endpoint prediction remains challenging for health providers. Although predictors such as age, gender, and disease staging are of considerable predictive value, the accuracy often ranges between 60 and 80%. An accurate prognosis assessment is required for making effective clinical decisions.
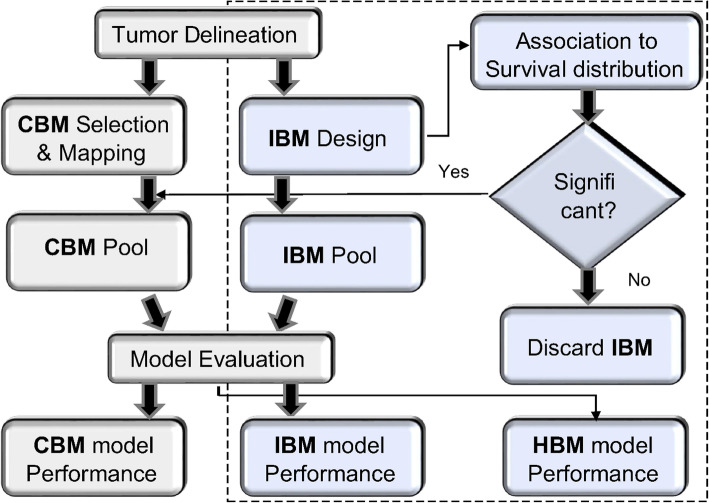
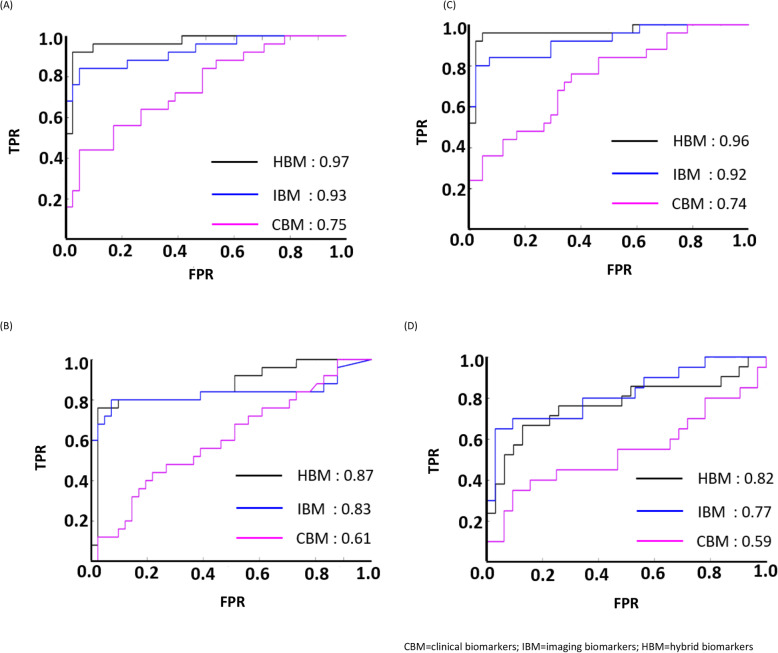
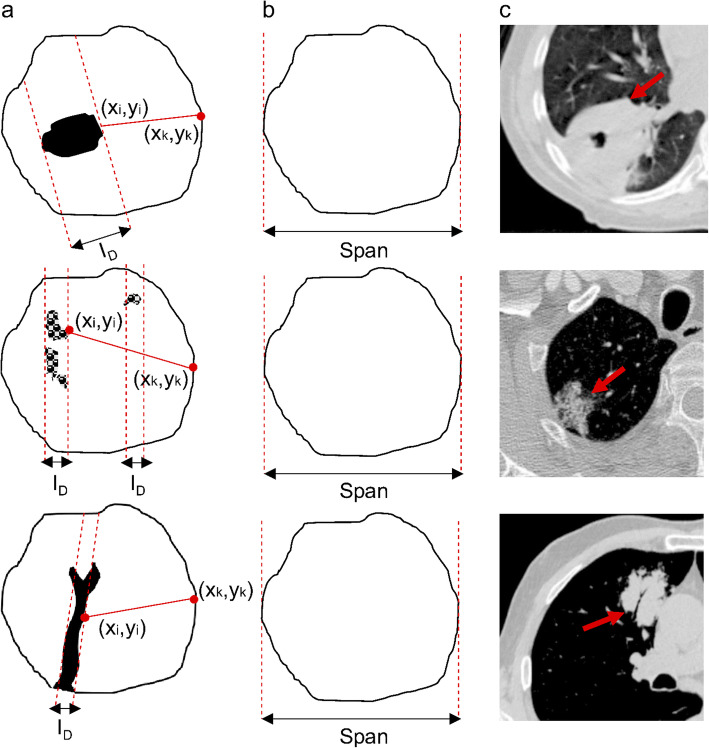
We proposed an extended prognostic model based on clinical covariates with adjustment for additional variables that were radio-graphically induced, termed imaging biomarkers. Eight imaging biomarkers were introduced and investigated in a cohort of 68 non-small cell lung cancer subjects with tumor internal characteristic. The subjects comprised of 40 males and 28 females with mean age at 68.7 years. The imaging biomarkers used to quantify the solid component and non-solid component of a tumor. The extended model comprises of additional frameworks that correlate these markers to the survival ends through uni- and multi-variable analysis to determine the most informative predictors, before combining them with existing clinical predictors. Performance was compared between traditional and extended approaches using Receiver Operating Characteristic (ROC) curves, Area under the ROC curves (AUC), Kaplan-Meier (KM) curves, Cox Proportional Hazard, and log-rank tests (p-value).
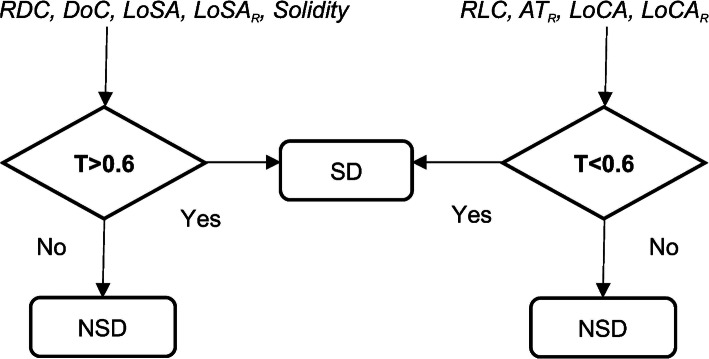
The proposed hybrid model exhibited an impressive boosting pattern over the traditional approach of prognostic modelling in the survival prediction (AUC ranging from 77 to 97%). Four developed imaging markers were found to be significant in distinguishing between subjects having more and less dense components: (P = 0.002-0.006). The correlation to survival analysis revealed that patients with denser composition of tumor (solid dominant) lived 1.6-2.2 years longer (mean survival) and 0.5-2.0 years longer (median survival), than those with less dense composition (non-solid dominant).
The present study provides crucial evidence that there is an added value for incorporating additional image-based predictors while predicting clinical endpoints. Though the hypotheses were confirmed in a customized case study, we believe the proposed model is easily adapted to various clinical cases, such as predictions of complications, treatment response, and disease evolution.
临床终点预测仍然是医疗服务提供者面临的挑战。虽然年龄、性别和疾病分期等预测因子具有相当大的预测价值,但准确性通常在 60%至 80%之间。为了做出有效的临床决策,需要进行准确的预后评估。
我们提出了一种基于临床协变量的扩展预后模型,并对影像学诱导的附加变量进行了调整,称为影像学生物标志物。在 68 名非小细胞肺癌患者的肿瘤内部特征的队列中引入并研究了 8 种影像学生物标志物。该队列包括 40 名男性和 28 名女性,平均年龄为 68.7 岁。这些影像学生物标志物用于量化肿瘤的实性成分和非实性成分。扩展模型包含了额外的框架,通过单变量和多变量分析将这些标志物与生存终点相关联,以确定最具信息量的预测因子,然后将它们与现有的临床预测因子相结合。通过接收者操作特征(ROC)曲线、ROC 曲线下面积(AUC)、Kaplan-Meier(KM)曲线、Cox 比例风险和对数秩检验(p 值)比较传统方法和扩展方法的性能。
与传统的预后建模方法相比,所提出的混合模型在生存预测方面表现出令人印象深刻的提升模式(AUC 范围从 77%到 97%)。发现四种开发的影像学标志物在区分具有更密集和更稀疏成分的患者方面具有显著差异:(P 值为 0.002-0.006)。与生存分析的相关性表明,肿瘤组成密度较高(实性为主)的患者的平均生存期延长了 1.6-2.2 年,中位生存期延长了 0.5-2.0 年,而肿瘤组成密度较低(非实性为主)的患者的平均生存期延长了 1.6-2.2 年。
本研究提供了重要证据,表明在预测临床终点时,结合额外的基于图像的预测因子具有附加价值。虽然在定制的案例研究中验证了假设,但我们相信所提出的模型很容易适应各种临床情况,如并发症预测、治疗反应和疾病演变。