Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, 100029, China.
Cardiovasc Diabetol. 2020 Oct 9;19(1):171. doi: 10.1186/s12933-020-01146-w.
Glycated albumin (GA) is a marker of short-term glycemic control and is strongly associated with the occurrence of diabetes. Previous studies have shown an association between GA and the effect of clopidogrel therapy on ischemic stroke. However, limited information is available regarding this relationship in acute coronary syndrome (ACS) patients. In this study, we evaluated the effect of GA on platelet P2Y12 inhibition by clopidogrel in patients with ACS.
Consecutive Chinese patients with ACS who received loading or maintenance doses of clopidogrel in addition to aspirin were recruited. At least 12 h after the patient had taken the clopidogrel dose, thromboelastography (TEG) and light transmittance aggregometry (LTA) were used to calculate the quantitative platelet inhibition rate to determine clopidogrel-induced antiplatelet reactivity. A prespecified cutoff of the maximum amplitude of adenosine diphosphate (ADP)-induced platelet-fibrin clot strength > 47 mm plus an ADP-induced platelet inhibition rate < 50% assessed by TEG or ADP-induced platelet aggregation > 40% assessed by LTA to indicate low responsiveness to clopidogrel were applied for evaluation. Patients were categorized into two groups based on a GA level of 15.5%, the cutoff point indicating the development of early-phase diabetes. Multivariate linear regression analysis was used to assess the interaction of GA with clopidogrel antiplatelet therapy.
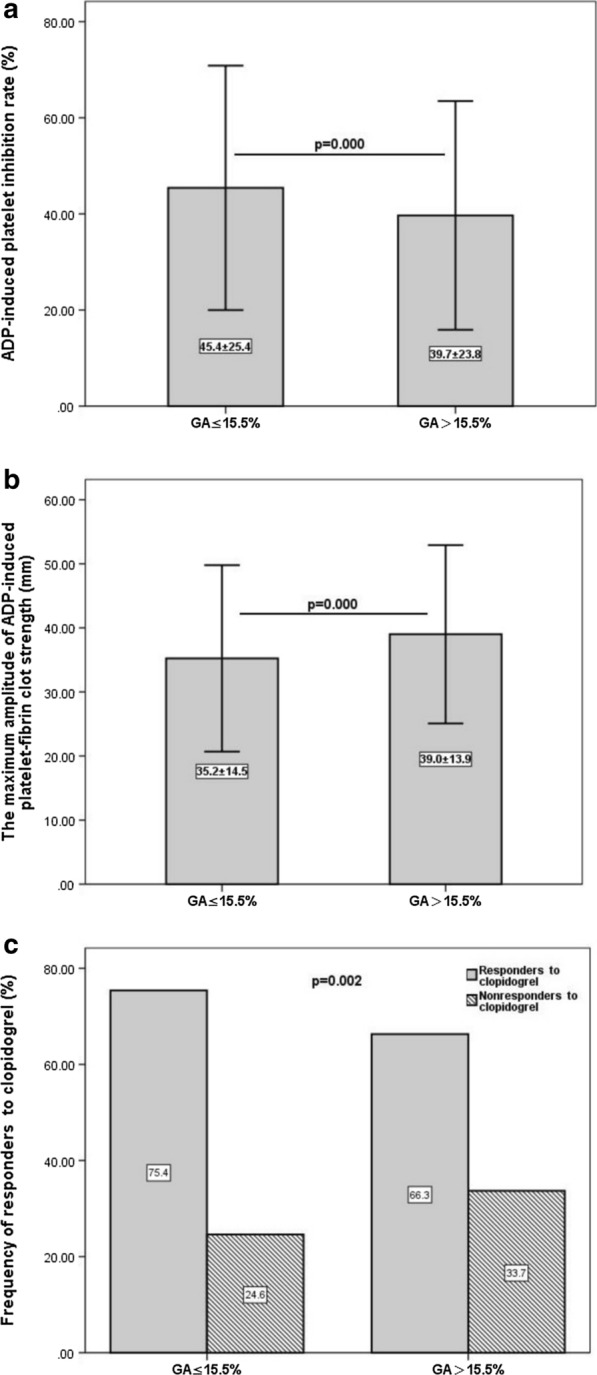
A total of 1021 participants were evaluated, and 28.3% of patients (289 of 1021) had low responsiveness to clopidogrel assessed by TEG. In patients with elevated GA levels, low responsiveness to clopidogrel assessed by TEG was observed in 33.7% (139 of 412) of patients, which was a significantly higher rate than that in the lower-GA-level group (24.6%, P = 0.002). According to multivariate linear regression analysis, a GA level > 15.5% was independently associated with low responsiveness to clopidogrel after adjustment for age, sex and other conventional confounding factors. This interaction was not mediated by a history of diabetes mellitus. A GA level ≤ 15.5% was associated with a high positive value [75.4%, 95% CI 73.0-77.6%] for predicting a normal responsiveness to clopidogrel.
GA could be a potential biomarker to predict the effects of clopidogrel antiplatelet therapy in ACS patients and might be a clinical biomarker to guide DAPT de-escalation.
糖化白蛋白(GA)是短期血糖控制的标志物,与糖尿病的发生密切相关。先前的研究表明,GA 与缺血性卒中患者氯吡格雷治疗效果之间存在关联。然而,关于急性冠状动脉综合征(ACS)患者中这种关系的信息有限。在本研究中,我们评估了 GA 对 ACS 患者氯吡格雷治疗中血小板 P2Y12 抑制的影响。
连续纳入了在中国接受氯吡格雷负荷或维持剂量治疗且加用阿司匹林的 ACS 患者。患者服用氯吡格雷至少 12 小时后,使用血栓弹力图(TEG)和光透射比浊法(LTA)计算血小板抑制率定量值,以确定氯吡格雷诱导的抗血小板反应。采用 TEG 检测到的最大振幅>47mm 加 ADP 诱导的血小板抑制率<50%,或 LTA 检测到的 ADP 诱导的血小板聚集>40%的预设截定点,提示对氯吡格雷的低反应性,用于评估。根据 GA 水平(15.5%,表示早期糖尿病发生的截定点)将患者分为两组。采用多变量线性回归分析评估 GA 与氯吡格雷抗血小板治疗的相互作用。
共评估了 1021 名患者,其中 28.3%(289/1021)的患者(根据 TEG 评估)对氯吡格雷的反应性较低。在 GA 水平升高的患者中,33.7%(412 例患者中的 139 例)根据 TEG 评估对氯吡格雷的反应性较低,这一比率明显高于 GA 水平较低的患者(24.6%,P=0.002)。根据多变量线性回归分析,GA 水平>15.5%在调整年龄、性别和其他常规混杂因素后与氯吡格雷低反应性独立相关。这种相互作用不受糖尿病史的影响。GA 水平≤15.5%与氯吡格雷高反应性的阳性预测值(75.4%,95%CI 73.0%-77.6%)密切相关。
GA 可能是预测 ACS 患者氯吡格雷抗血小板治疗效果的潜在生物标志物,可能是指导 DAPT 降级的临床生物标志物。