Neurology Clinic, University of Perugia-S. Maria della Misericordia Hospital, Perugia, Italy.
Neurology Unit, Rimini "Infermi" Hospital-AUSL Romagna, Viale Settembrini 2, 47923, Rimini, Italy.
Neurol Sci. 2021 Jun;42(6):2301-2308. doi: 10.1007/s10072-020-04735-5. Epub 2020 Oct 10.
Despite intravenous thrombolysis (IVT) and endovascular treatment (EVT) have been demonstrated effective in acute ischemic stroke (AIS) due to large vessel occlusions, there are still no conclusive data to guide treatment in stroke due to cervical internal carotid artery (ICA) occlusion. We systematically reviewed available literature to compare IVT, EVT, and bridging (IVT + EVT) and define optimal treatment.
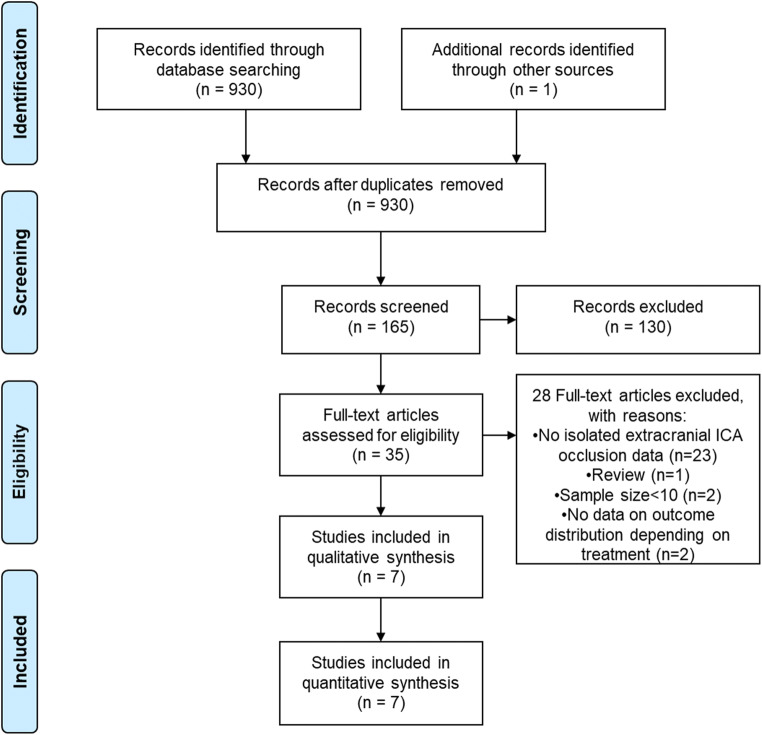
Systematic review followed predefined protocol (Open-Science-Framework osf.io/bfykj ). MEDLINE, EMBASE, and Cochrane CENTRAL were searched. Results were restricted to studies in English, with sample size ≥ 10 and follow-up ≥30 days. Primary outcomes were favorable outcome (mRS ≤ 2), mortality, and symptomatic intracerebral hemorrhage(sICH), defined according to study original report. Newcastle-Ottawa scale was used for bias assessment.
Seven records of 930 screened were included in meta-analysis. Quality of studies was low-to-fair in 5, good in 2. IVT (n = 450) did not differ for favorable outcome and mortality compared to EVT (n = 150), though having lower rate of sICH (OR = 0.4, 95% CI 0.2-0.8). Compared to IVT, bridging (IVT + EVT) was associated with higher rate of favorable outcome (OR = 2.2, 95% CI 1.3-3.7). Compared to EVT, bridging (IVT + EVT) provided higher rate of favorable outcome (OR = 1.9, 95% CI 1.1-3.4), with a marginally increased risk of sICH (OR = 2.1, 95% CI 1-4.4) but similar mortality rates.
Our systematic review highlights that, in acute ischemic stroke associated with isolated cervical ICA occlusion, bridging (IVT + EVT) might lead to higher rate of functional independence at follow-up, without increasing mortality. The low quality of available studies prevents from drawing firm conclusions, and randomized-controlled clinical trials are critically needed to define optimal treatment in this AIS subgroup.
尽管静脉溶栓(IVT)和血管内治疗(EVT)已被证明对大动脉闭塞引起的急性缺血性脑卒中(AIS)有效,但对于颈内动脉(ICA)闭塞引起的脑卒中,仍没有确凿的数据来指导治疗。我们系统地回顾了现有文献,比较了 IVT、EVT 和桥接(IVT+EVT),并确定了最佳治疗方法。
遵循预设方案进行系统评价(Open-Science-Framework osf.io/bfykj)。检索 MEDLINE、EMBASE 和 Cochrane CENTRAL。结果仅限于英语研究,样本量≥10,随访≥30 天。主要结局是良好结局(mRS≤2)、死亡率和症状性颅内出血(sICH),根据研究原始报告定义。使用纽卡斯尔-渥太华量表评估偏倚。
在筛选的 930 条记录中,有 7 条记录纳入了荟萃分析。5 项研究的质量为低至中等,2 项研究的质量良好。与 EVT(n=150)相比,IVT(n=450)在良好结局和死亡率方面没有差异,但 sICH 发生率较低(OR=0.4,95%CI 0.2-0.8)。与 IVT 相比,桥接(IVT+EVT)与良好结局发生率较高相关(OR=2.2,95%CI 1.3-3.7)。与 EVT 相比,桥接(IVT+EVT)提供了更高的良好结局率(OR=1.9,95%CI 1.1-3.4),sICH 风险略有增加(OR=2.1,95%CI 1-4.4),但死亡率相似。
我们的系统综述强调,在孤立性颈内动脉闭塞引起的急性缺血性脑卒中患者中,桥接(IVT+EVT)可能会提高随访时的功能独立性,而不会增加死亡率。现有研究的质量较低,无法得出确凿的结论,需要进行随机对照临床试验来确定该 AIS 亚组的最佳治疗方法。