Department of Economics and Related Studies, University of York, York, UK
Centre for Health Economics, University of York, York, UK.
BMJ Open. 2020 Oct 10;10(10):e036411. doi: 10.1136/bmjopen-2019-036411.
The UK government is proposing to cease cutting the local authority public health grant by reallocating part of the treatment budget to preventative activity. This study examines whether this proposal is evidenced based and, in particular, whether these resources are best reallocated to prevention, or whether this expenditure would generate more health gains if used for treatment.
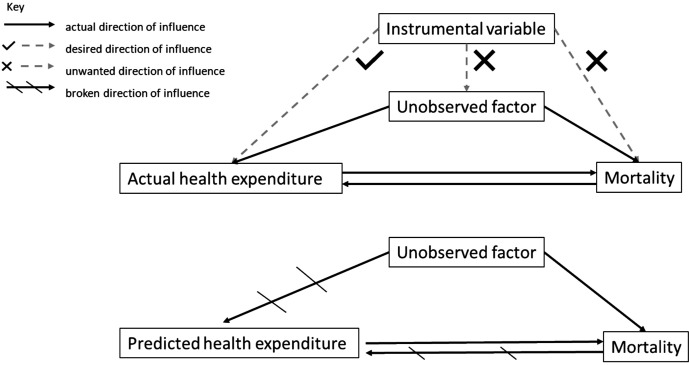
Instrumental variable regression methods are applied to English local authority data on mortality, healthcare and public health expenditure to estimate the responsiveness of mortality to variations in healthcare and public health expenditure in 2013/14. Using a well-established method, these mortality results are converted to a quality-adjusted life year (QALY) basis, and this facilitates the estimation of the cost per QALY for both National Health Service (NHS) healthcare and local public health expenditure.
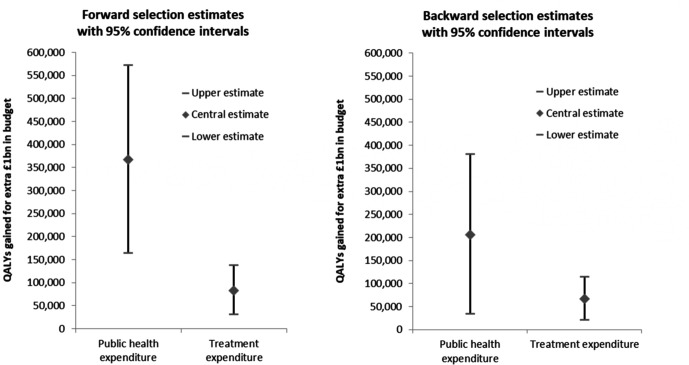
Saving lives and improving the quality of life requires resources. Our estimates suggest that each additional QALY costs about £3800 from the local public health budget, and that each additional QALY from the NHS budget costs about £13 500. These estimates can be used to calculate the number of QALYs generated by a budget boost. If we err on the side of caution and use the most conservative estimates that we have, then an additional £1 billion spent on public health will generate 206 398 QALYs (95% CI 36 591 to 3 76 205 QALYs), and an additional £1 billion spent on healthcare will generate 67 060 QALYs (95% CI 21 487 to 112 633 QALYs).
Additional public health expenditure is very productive of health and is more productive than additional NHS expenditure. However, both types of expenditure are more productive of health than the norms used by National Institute for Health and Care Excellence (£20 000-£30 000 per QALY) to judge whether new therapeutic technologies are suitable for adoption by the NHS.
英国政府提议停止削减地方当局公共卫生拨款,将部分治疗预算重新分配给预防活动。本研究旨在检验这一提案是否有证据支持,特别是这些资源是否最好重新分配给预防,或者如果将这些支出用于治疗,是否会带来更多的健康收益。
利用英格兰地方当局关于死亡率、医疗保健和公共卫生支出的数据,采用工具变量回归方法,估计 2013/14 年医疗保健和公共卫生支出变化对死亡率的反应。利用一种成熟的方法,将这些死亡率结果转换为质量调整生命年(QALY)基础,从而便于估计国民保健服务(NHS)医疗保健和地方公共卫生支出的每 QALY 成本。
拯救生命和提高生活质量需要资源。我们的估计表明,从地方公共卫生预算中每增加一个 QALY 需要花费约 3800 英镑,从 NHS 预算中每增加一个 QALY 需要花费约 13500 英镑。这些估计可用于计算预算增加带来的 QALY 数量。如果我们谨慎行事,使用我们拥有的最保守的估计,那么额外花费 10 亿英镑用于公共卫生将产生 206398 个 QALY(95%CI 36591 至 376205 QALY),额外花费 10 亿英镑用于医疗保健将产生 67060 个 QALY(95%CI 21487 至 112063 QALY)。
额外的公共卫生支出对健康非常有成效,比额外的 NHS 支出更有成效。然而,与国民保健卓越研究所(NICE)用于判断新的治疗技术是否适合 NHS 采用的标准(每 QALY 20000-30000 英镑)相比,这两种类型的支出都更能提高健康水平。