University of Massachusetts, Department of Orthopaedic Surgery, Worcester MA, United States of America.
University of Massachusetts, Department of Orthopaedic Surgery, Worcester MA, United States of America.
Injury. 2021 Jun;52(6):1522-1528. doi: 10.1016/j.injury.2020.10.018. Epub 2020 Oct 5.
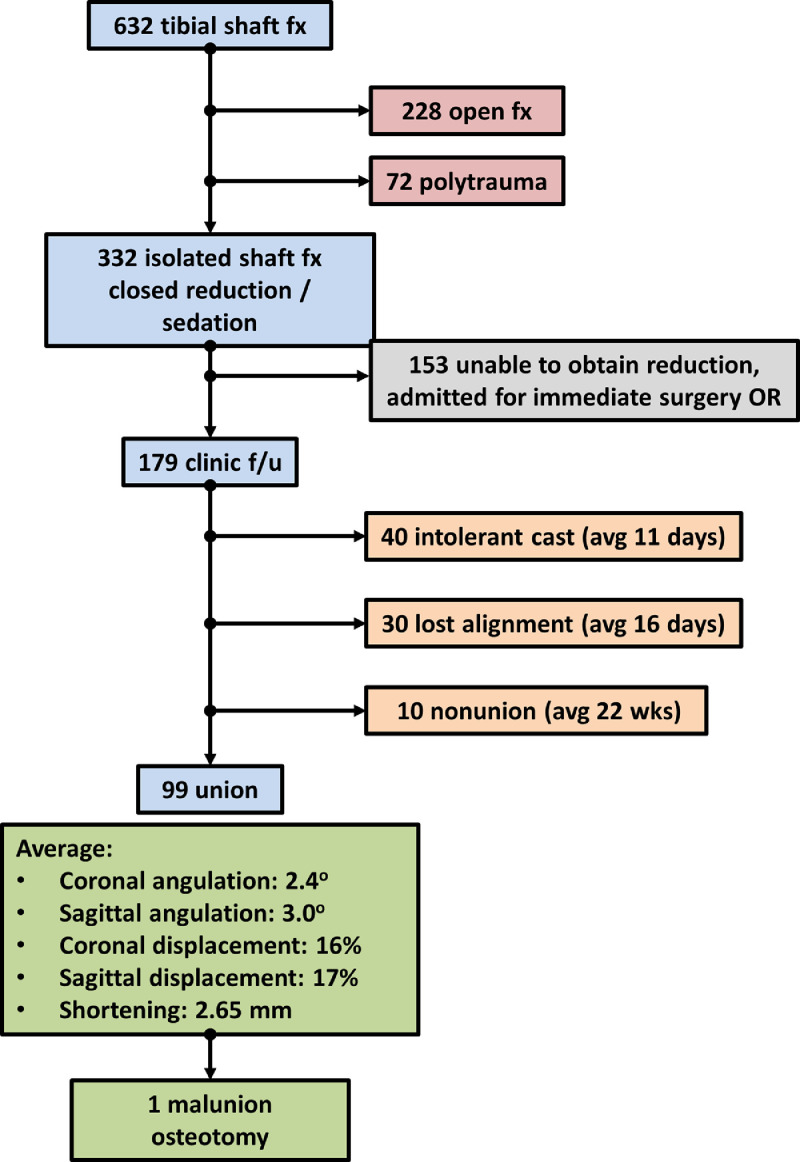
The decision to attempt closed treatment on tibial shaft fractures can be challenging. At our institution, we attempt treatment of nearly all closed, isolated tibial shaft fractures. The purpose of this study was to report the results of 10 years of experience to develop a tool to identify patients for whom non-operative treatment of tibial shaft fractures may be a viable option METHOD: This was a retrospective review of patients with tibial shaft fracture seen at a level 1 trauma center over 10 years. Patients with closed, isolated injuries underwent sedation, closed reduction, long-leg casting, and outpatient follow-up. Patients were converted to surgery for inability to obtain or maintain acceptable alignment or patient intolerance. Radiographic characteristics and patient demographics were extracted. Logistic regression analysis was used to develop a model to predict which patient and injury characteristics determined success of nonoperative treatment.
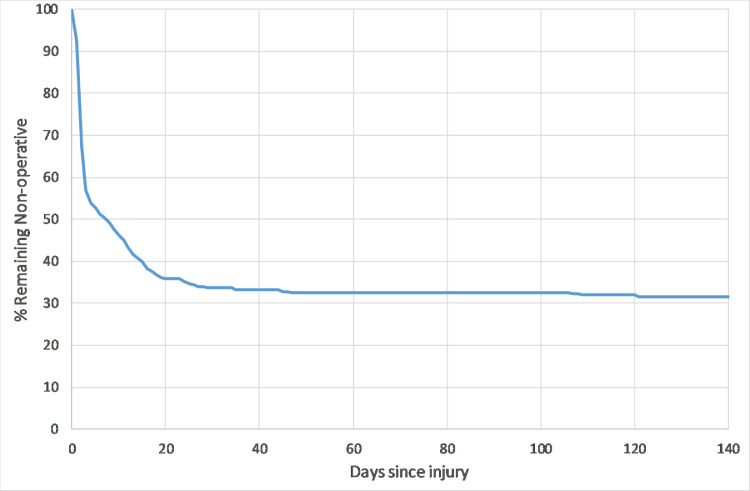
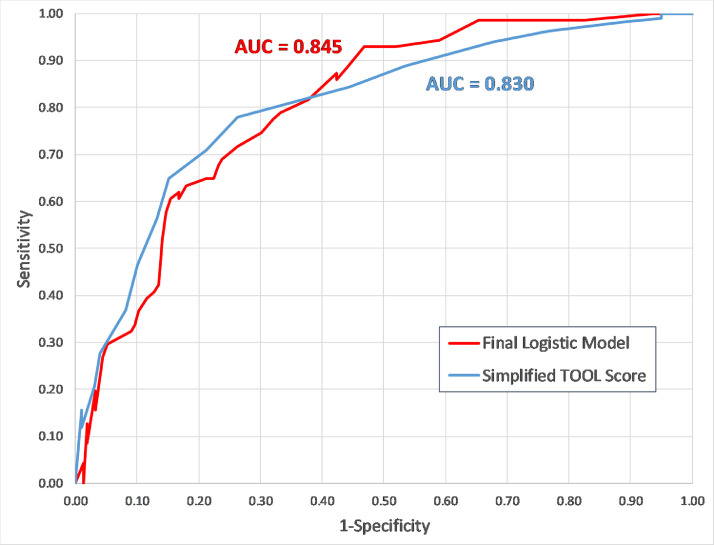
334 patients were identified with isolated, closed tibial shaft fractures, who were reduced and treated in a long leg cast. 234 patients (70%) converted to surgical treatment due to inability to maintain alignment, patient intolerance, and nonunion. In a regression model, coronal/sagittal translation, sagittal angulation, fracture morphology, and smoking status were shown to be significant predictors of success of nonoperative treatment (p < 0.05). We developed a Tibial Operative Outcome Likelihood (TOOL) score designed to help predict success or failure of closed treatment. The TOOL score can be used to identify a subsegment of patients with injuries amenable to closed treatment (38% of injuries) with a nonoperative success rate over 60%.
Non-operative treatment of tibial shaft fractures is feasible, although there is a relatively high conversion rate to operative treatment. However, it is possible to use injury characteristics to identify a cohort of patients with a higher chance of success with closed treatment, which is potentially useful in a resource-constrained setting or for patients who wish to avoid surgery.
Prognostic Level 3.
尝试闭合治疗胫骨骨干骨折的决策具有挑战性。在我们的机构中,我们尝试治疗几乎所有闭合性、孤立性胫骨骨干骨折。本研究的目的是报告 10 年经验的结果,以开发一种工具,以确定非手术治疗胫骨骨干骨折可能是可行选择的患者。
这是对 10 年来在 1 级创伤中心就诊的胫骨骨干骨折患者的回顾性研究。闭合性、孤立性损伤的患者接受镇静、闭合复位、长腿石膏固定和门诊随访。对于无法获得或维持可接受的对线或患者不耐受的患者,转换为手术治疗。提取患者的影像学特征和人口统计学资料。使用逻辑回归分析来建立一个模型,以预测哪些患者和损伤特征决定非手术治疗的成功。
确定了 334 例孤立性、闭合性胫骨骨干骨折患者,他们接受了复位和长腿石膏固定治疗。234 例(70%)由于无法维持对线、患者不耐受和不愈合而转换为手术治疗。在回归模型中,冠状/矢状面平移、矢状面成角、骨折形态和吸烟状况被证明是非手术治疗成功的显著预测因素(p<0.05)。我们开发了一个胫骨手术结果可能性(TOOL)评分,旨在帮助预测闭合治疗的成功或失败。TOOL 评分可用于识别具有闭合治疗适应证的亚段患者(38%的损伤),非手术成功率超过 60%。
胫骨骨干骨折的非手术治疗是可行的,尽管手术治疗的转化率相对较高。然而,使用损伤特征来识别具有更高闭合治疗成功率的患者队列是可能的,这在资源有限的环境中或对于希望避免手术的患者可能是有用的。
预后 3 级。