Department of Surgery and Legal Medicine, Psychiatry and Pathology, School of Medicine, Complutense University of Madrid; Department of Pathology, Hospital Clínico San Carlos, Madrid, Spain.
Department of Pathology, Hospital Rey Juan Carlos; Department of Basic Medical Sciences, School of Medicine, Rey Juan Carlos University, Madrid, Spain.
Saudi J Gastroenterol. 2021 Jan-Feb;27(1):44-53. doi: 10.4103/sjg.SJG_208_20.
Factors other than pTNM stage have been associated with gastric cancer (GC) prognosis, and several alternative prognostic scores have been constructed. Our aims are to identify prognostic factors in western GC patients and to build clinicopathological prognostic models for overall survival (OS) and disease-free survival (DFS).
A Retrospective study of 204 cases of GC resected during the years 2000 to 2014 was conducted in our hospital. Clinicopathological features were assessed, univariate and multivariate analysis were performed and prognostic scores were constructed.
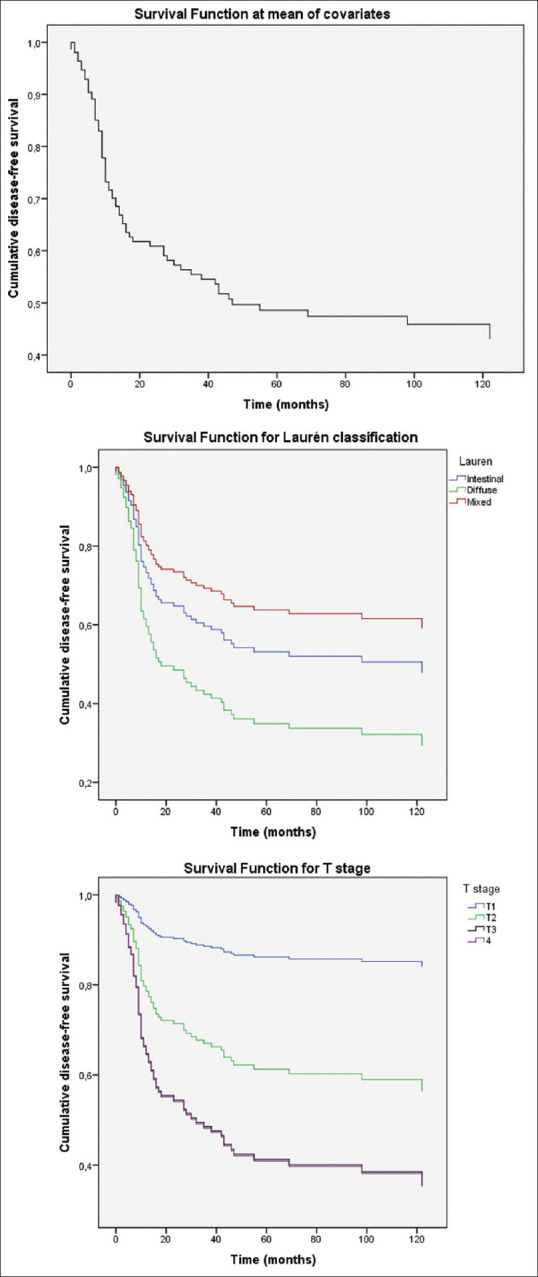
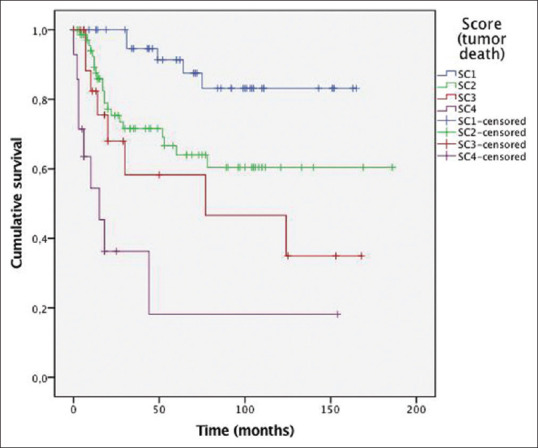
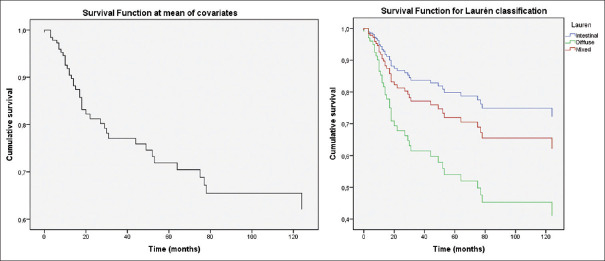
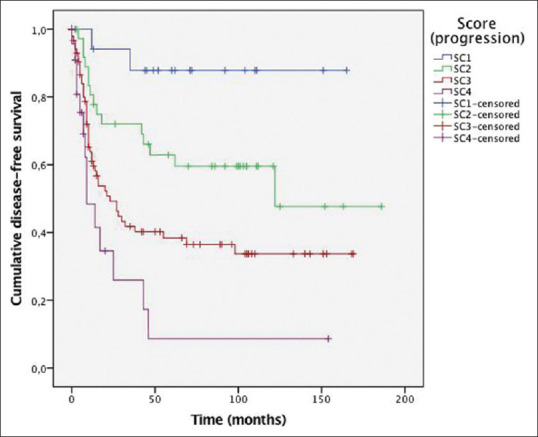
Most patients were diagnosed at pTNM stages II and III (36.9% and 48.1%, respectively). According to Laurén classification, tumors were intestinal (55.8%), diffuse (35.2%) and mixed (9%). During follow-up, 43.5% of patients had tumor recurrence, and 28.6% died due to tumor. Univariate analysis showed that patient age, Laurén subtype, signet-ring cell morphology, pTNM stage, tumor grade, perineural invasion, growth pattern, intratumoral inflammation, adjuvant therapy, and desmoplasia were significantly related to tumor progression or death. Multivariate analysis showed that Laurén subtype, pT stage, and lymph node ratio (LNR) were significantly and independently associated with GC recurrence. Laurén subtype and LNR were significantly related to patient survival. Prognostic scores for tumor progression and death were developed and patients were classified into four prognostic groups which showed good prognostic performance.
A prognostic model comprising histological features such as Laurén subtype can be easily applied in clinical practice, and provides more prognostic information than pTNM stage alone. These models can further stratify resected GC patients and have the potential to aid in the individualization of patient management.
除 pTNM 分期外,其他因素与胃癌(GC)预后相关,已构建了几种替代预后评分。我们的目的是确定西方 GC 患者的预后因素,并构建用于总生存(OS)和无病生存(DFS)的临床病理预后模型。
对 2014 年期间在我院接受 GC 切除术的 204 例患者进行回顾性研究。评估了临床病理特征,进行了单因素和多因素分析,并构建了预后评分。
大多数患者被诊断为 pTNM 分期 II 期和 III 期(分别为 36.9%和 48.1%)。根据Laurén 分类,肿瘤为肠型(55.8%)、弥漫型(35.2%)和混合型(9%)。在随访期间,43.5%的患者发生肿瘤复发,28.6%的患者因肿瘤死亡。单因素分析显示,患者年龄、Laurén 亚型、印戒细胞形态、pTNM 分期、肿瘤分级、神经周围侵犯、生长模式、肿瘤内炎症、辅助治疗和纤维增生与肿瘤进展或死亡显著相关。多因素分析显示,Laurén 亚型、pT 分期和淋巴结比值(LNR)与 GC 复发显著且独立相关。Laurén 亚型和 LNR 与患者生存显著相关。建立了用于肿瘤进展和死亡的预后评分,并将患者分为四个预后组,显示出良好的预后性能。
包含组织学特征(如 Laurén 亚型)的预后模型可在临床实践中轻松应用,并提供比单独 pTNM 分期更多的预后信息。这些模型可进一步对接受切除术的 GC 患者进行分层,并有可能帮助患者个体化管理。