Hoshina Tokio, Aonuma Hiroka, Ote Manabu, Sakurai Tatsuya, Saiki Erisha, Kinjo Yuki, Kondo Kazuhiro, Okabe Masataka, Kanuka Hirotaka
Team COVID-19 PCR Center, The Jikei University School of Medicine, 3-25-8, Nishi-Shinbashi, Minato-ku, Tokyo, 105-8461 Japan.
Department of Infectious Diseases and Infection Control, The Jikei University School of Medicine, 3-25-8, Nishi-Shinbashi, Minato-ku, Tokyo, 105-8461 Japan.
Inflamm Regen. 2020 Oct 12;40:38. doi: 10.1186/s41232-020-00147-2. eCollection 2020.
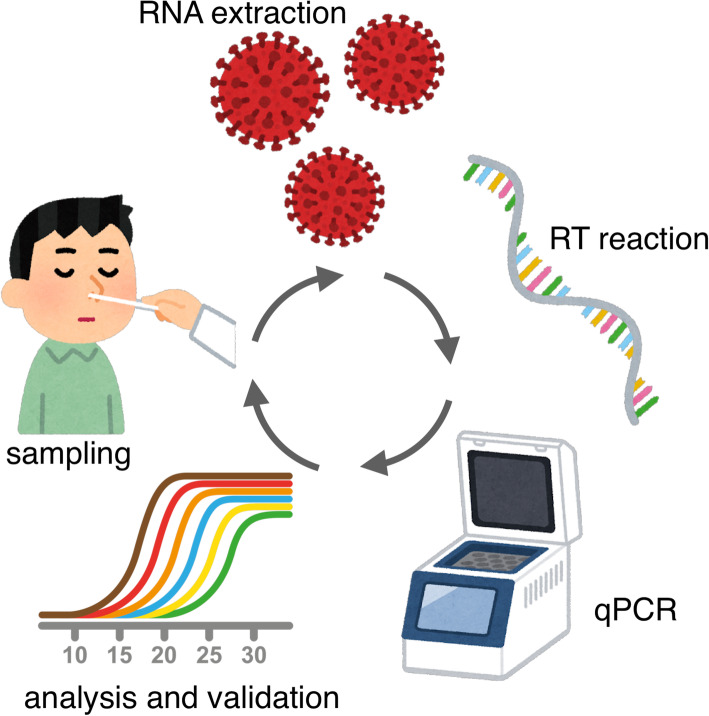
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first emerged in Wuhan, China, and has spread globally to most countries. In Japan, the first COVID-19 patient was identified on January 15, 2020. By June 30, the total number of patients diagnosed with COVID-19 reached 18,000. The impact of molecular detection of pathogens is significant in acute-care settings where rapid and accurate diagnostic measures are critical for decisions in patient treatment and outcomes of infectious diseases. Polymerase chain reaction (PCR)-based methods, such as quantitative PCR (qPCR), are the most established gene amplification tools and have a comprehensive range of clinical applications, including detecting a variety of pathogens, even novel agents causing emerging infections. Because SARS-CoV-2 contains a single-stranded RNA genome, reverse-transcription qPCR (RT-qPCR) has been broadly employed for rapid and sensitive quantitative measurements of viral RNA copy numbers. The RT-qPCR method, however, still requires time-consuming reactions with two different enzymes in addition to isolation of RNA from patient samples, limiting the numbers of testing institutions for diagnosing SARS-CoV-2 infection. Japan is known to have performed a relatively small number of PCR tests as well as confirmed cases among developed nations; as of June 30, 2020, approximately 390,000 people in Japan had undergone PCR tests. Given the devastating impact on medical services and the scale of demand for diagnostic testing of COVID-19, it has been proposed that academic settings such as basic research departments in university/college can be engaged in diagnosing, especially in university hospitals or academic medical centers. In collaboration with established diagnostic laboratories, academic facilities can divert their function to detecting virus from patients with suspected COVID-19, adopting existing specialized expertise in virus handling, molecular work, and data analysis. This in-house testing strategy facilitates the rapid diagnosing of thousands of samples per day and reduces sample turnaround time from 1 week to less than 24 h. This review provides an overview of the general principles, diagnostic value, and limitations of COVID-19 diagnosis platforms in Japan, in particular in-house testing at academic settings.
2019冠状病毒病(COVID-19)由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引起,最初在中国武汉出现,并已在全球传播至大多数国家。在日本,首例COVID-19患者于2020年1月15日被确诊。截至6月30日,日本确诊的COVID-19患者总数达到18000例。在急诊环境中,病原体的分子检测具有重要意义,因为快速准确的诊断措施对于患者治疗决策和传染病的转归至关重要。基于聚合酶链反应(PCR)的方法,如定量PCR(qPCR),是最成熟的基因扩增工具,具有广泛的临床应用,包括检测各种病原体,甚至是导致新出现感染的新型病原体。由于SARS-CoV-2含有单链RNA基因组,逆转录qPCR(RT-qPCR)已被广泛用于病毒RNA拷贝数的快速灵敏定量测定。然而,RT-qPCR方法除了需要从患者样本中分离RNA外,仍需要使用两种不同的酶进行耗时的反应,这限制了诊断SARS-CoV-2感染的检测机构数量。在发达国家中,日本进行的PCR检测数量以及确诊病例数相对较少;截至2020年6月30日,日本约有39万人接受了PCR检测。鉴于COVID-19对医疗服务造成的毁灭性影响以及诊断检测的需求规模,有人提议大学/学院的基础研究部门等学术机构可以参与诊断工作,特别是在大学医院或学术医疗中心。通过与成熟的诊断实验室合作,学术机构可以将其功能转向检测疑似COVID-19患者的病毒,利用现有的病毒处理、分子操作和数据分析方面的专业知识。这种内部检测策略有助于每天快速诊断数千个样本,并将样本周转时间从1周缩短至不到24小时。本综述概述了日本COVID-19诊断平台的一般原则、诊断价值和局限性,特别是学术机构的内部检测情况。