Katahira Masato, Hirama Takashi, Eba Shunsuke, Suzuki Takaya, Notsuda Hirotsugu, Oishi Hisashi, Matsuda Yasushi, Sado Tetsu, Noda Masafumi, Sakurada Akira, Sidhu Aman, Okada Yoshinori
Department of Thoracic Surgery, Institute of Development, Aging and Cancer, Tohoku University, Sendai, Miyagi, Japan.
Division of Organ Transplantation, Tohoku University Hospital, Sendai, Miyagi, Japan.
Transplant Direct. 2020 May 28;6(6):e562. doi: 10.1097/TXD.0000000000001013. eCollection 2020 Jun.
Acute kidney injury (AKI) is a common complication after lung transplant (LTx), and continuous renal replacement therapy (CRRT) is increasingly of use to critically ill patients who have developed AKI. However, the optimal timing or threshold of kidney impairment for which to commence CRRT after LTx has been uncertain. There has also been limited information on the impact of CRRT among LTx recipients (LTRs) introduced in the early posttransplant period on survival, graft function, and renal function. We aimed to review LTRs who developed AKI requiring CRRT postoperatively and followed their long-term outcomes at Tohoku University Hospital (TUH).
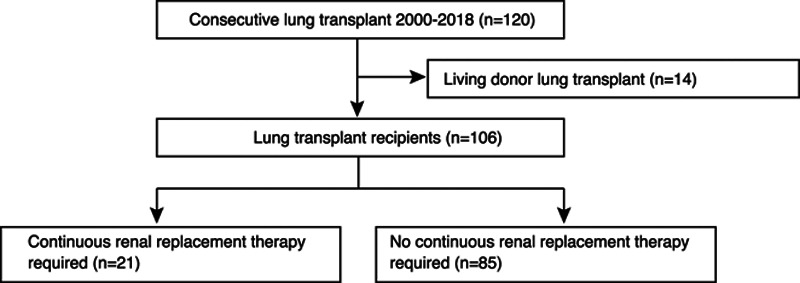
Medical records of consecutive patients who underwent LTx at TUH between 2000 and 2018 were reviewed, with follow-up to 2019 inclusive.
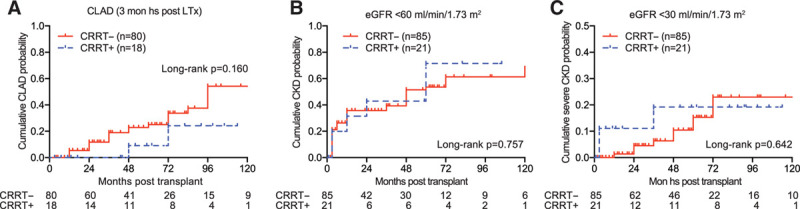
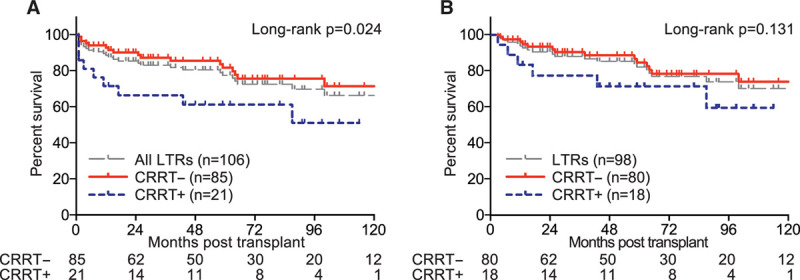
Although mortality in those who required CRRT (n = 21) was increased versus those who did not require CRRT (n = 85)( = 0.024), conditional survival beyond 3-month posttransplant was not affected ( = 0.131). Additionally, the cumulative incidence of chronic lung allograft rejection ( = 0.160) and the development of chronic kidney disease ( = 0.757) were not significant between groups.
The initiation of CRRT posttransplant may be a useful strategy to preserve cardiac and optimize volume management among critically ill patients.
急性肾损伤(AKI)是肺移植(LTx)术后常见的并发症,连续性肾脏替代治疗(CRRT)越来越多地用于发生AKI的危重病患者。然而,LTx术后开始CRRT的最佳时机或肾脏损害阈值尚不确定。关于移植后早期引入CRRT对肺移植受者(LTRs)的生存、移植物功能和肾功能的影响,相关信息也有限。我们旨在回顾在东北大学医院(TUH)术后发生需要CRRT的AKI的LTRs,并跟踪其长期预后。
回顾了2000年至2018年在TUH接受LTx的连续患者的病历,随访至2019年(含2019年)。
尽管需要CRRT的患者(n = 21)的死亡率高于不需要CRRT的患者(n = 85)(P = 0.024),但移植后3个月后的条件生存率不受影响(P = 0.131)。此外,两组之间慢性肺移植排斥反应的累积发生率(P = 0.160)和慢性肾脏病的发生情况(P = 0.757)均无显著差异。
移植后开始CRRT可能是一种有用的策略,可用于危重病患者的心脏保护和优化容量管理。