Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia.
Centre for Biostatistics and Clinical Trials, Peter MacCallum Cancer Centre, Melbourne, Australia.
Int J Radiat Oncol Biol Phys. 2021 Mar 1;109(3):756-763. doi: 10.1016/j.ijrobp.2020.10.011. Epub 2020 Oct 15.
Fewer attendances for radiation therapy results in increased efficiency and less foot traffic within a radiation therapy department. We investigated outcomes after single-fraction (SF) stereotactic body radiation therapy (SBRT) in patients with oligometastatic disease.
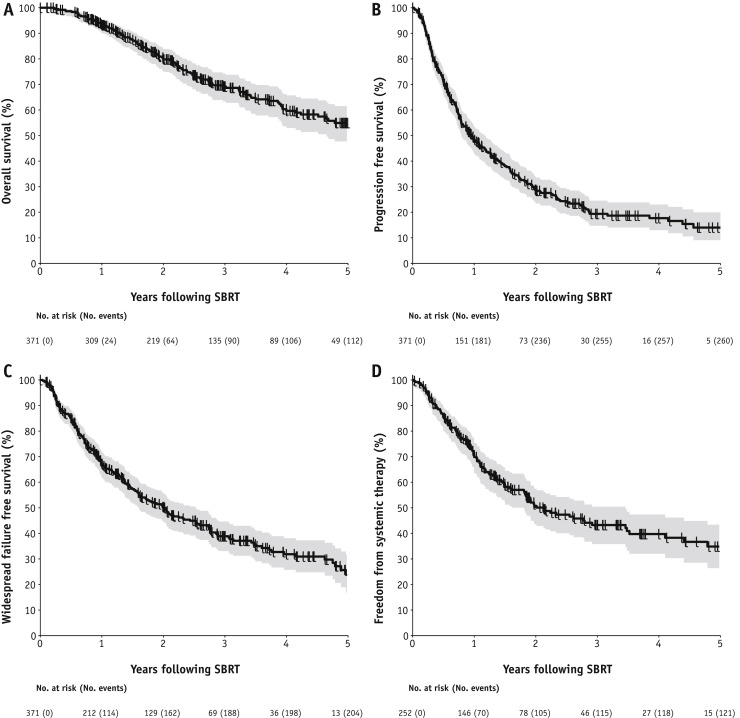
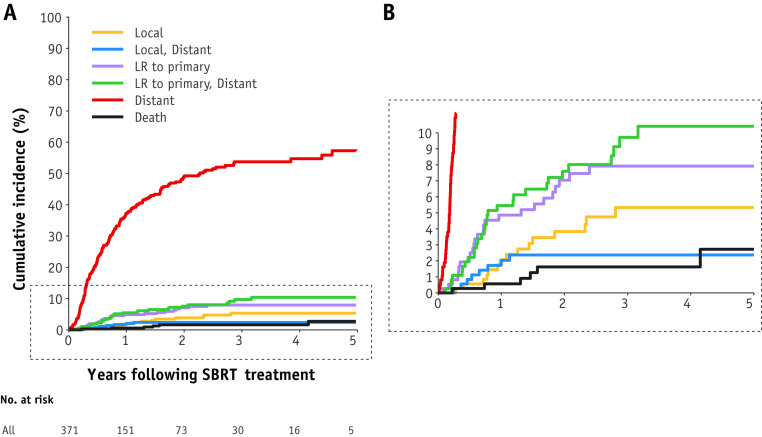
Between February 2010 and June 2019, patients who received SF SBRT to 1 to 5 sites of oligometastatic disease were included in this retrospective study. The primary objective was to describe patterns of first failure after SBRT. Secondary objectives included overall survival (OS), progression-free survival (PFS), high-grade treatment-related toxicity (Common Terminology Criteria for Adverse Events grade ≥3), and freedom from systemic therapy (FFST).
In total, 371 patients with 494 extracranial oligometastases received SF SBRT ranging from 16 Gy to 28 Gy. The most common primary malignancies were prostate (n = 107), lung (n = 63), kidney (n = 52), gastrointestinal (n = 51), and breast cancers (n = 42). The median follow-up was 3.1 years. The 1-, 3-, and 5-year OS was 93%, 69%, and 55%, respectively; PFS was 48%, 19%, and 14%, respectively; and FFST was 70%, 43%, and 35%, respectively. Twelve patients (3%) developed grade 3 to 4 treatment-related toxicity, with no grade 5 toxicity. As the first site of failure, the cumulative incidence of local failure (irrespective of other failures) at 1, 3 and 5 years was 4%, 8%, and 8%, respectively; locoregional relapse at the primary was 10%, 18%, and 18%, respectively; and distant failure was 45%, 66%, and 70%, respectively.
SF SBRT is safe and effective, and a significant proportion of patients remain FFST for several years after therapy. This approach could be considered in resource-constrained or bundled-payment environments. Locoregional failure of the primary site is the second most common pattern of failure, suggesting a role for optimization of primary control during metastasis-directed therapy.
放疗次数减少可提高放疗部门的效率并减少人员流动。我们研究了寡转移疾病患者单次分割立体定向放疗(SBRT)后的结果。
在 2010 年 2 月至 2019 年 6 月期间,对接受 1 至 5 个寡转移部位 SBRT 的患者进行了这项回顾性研究。主要目标是描述 SBRT 后首次失败的模式。次要目标包括总生存率(OS)、无进展生存率(PFS)、高级别治疗相关毒性(不良事件通用术语标准 3 级及以上)和无系统治疗(FFST)。
共 371 例 494 例颅外寡转移患者接受了 16Gy 至 28Gy 的单次分割 SBRT。最常见的原发恶性肿瘤为前列腺癌(n = 107)、肺癌(n = 63)、肾癌(n = 52)、胃肠道癌(n = 51)和乳腺癌(n = 42)。中位随访时间为 3.1 年。1、3 和 5 年 OS 分别为 93%、69%和 55%;PFS 分别为 48%、19%和 14%;FFST 分别为 70%、43%和 35%。12 例(3%)发生 3 至 4 级治疗相关毒性,无 5 级毒性。作为首次失败部位,1、3 和 5 年局部失败(无论其他失败)的累积发生率分别为 4%、8%和 8%;原发性局部区域复发率分别为 10%、18%和 18%;远处失败率分别为 45%、66%和 70%。
单次分割 SBRT 安全有效,治疗后数年仍有相当比例的患者保持 FFST。在资源有限或捆绑支付环境中,可以考虑这种方法。原发性部位的局部区域复发是第二常见的失败模式,这表明在转移性疾病定向治疗中优化原发性控制可能发挥作用。