Columbia University Vagelos College of Physicians and Surgeons, New York City, New York.
New York Presbyterian Hospital, New York City, New York.
Ann Surg. 2021 Jan 1;273(1):34-40. doi: 10.1097/SLA.0000000000004420.
To evaluate the perioperative morbidity and mortality of patients with COVID-19 who undergo urgent and emergent surgery.
Although COVID-19 infection is usually associated with mild disease, it can lead to severe respiratory complications. Little is known about the perioperative outcomes of patients with COVID-19.
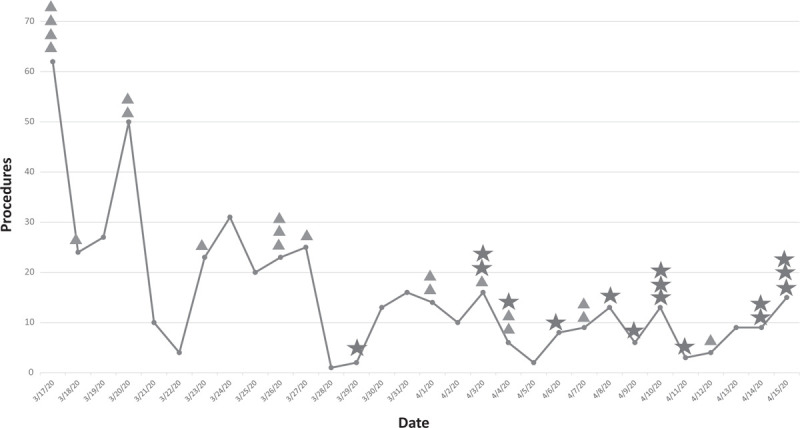
We examined patients who underwent urgent and emergent surgery at 2 hospitals in New York City from March 17 to April 15, 2020. Elective surgical procedures were cancelled throughout and routine, laboratory based COVID-19 screening was instituted on April 1. Mortality, complications, and admission to the intensive care unit were compared between patients with COVID-19 detected perioperatively and controls.
Among 468 subjects, 36 (7.7%) had confirmed COVID-19. Among those with COVID-19, 55.6% were detected preoperatively and 44.4% postoperatively. Before the routine preoperative COVID-19 laboratory screening, 7.7% of cases were diagnosed preoperatively compared to 65.2% after institution of screening (P = 0.0008). The perioperative mortality rate was 16.7% in those with COVID-19 compared to 1.4% in COVID-19 negative subjects [aRR = 9.29; 95% confidence interval (CI), 5.68-15.21]. Serious complications were identified in 58.3% of COVID-19 subjects versus 6.0% of controls (aRR = 7.02; 95%CI, 4.96-9.92). Cardiac arrest, sepsis/shock, respiratory failure, pneumonia, acute respiratory distress syndrome, and acute kidney injury were more common in those with COVID-19. The intensive care unit admission rate was 36.1% in those with COVID-19 compared to 16.4% of controls (aRR = 1.34; 95%CI, 0.86-2.09).
COVID-19 is associated with an increased risk for serious perioperative morbidity and mortality. A substantial number of patients with COVID-19 are not identified until after surgery.
评估 COVID-19 患者行紧急和急诊手术的围手术期发病率和死亡率。
虽然 COVID-19 感染通常与轻症相关,但它可导致严重的呼吸道并发症。对于 COVID-19 患者的围手术期结局,我们知之甚少。
我们检查了 2020 年 3 月 17 日至 4 月 15 日期间在纽约市 2 家医院接受紧急和急诊手术的患者。整个期间取消了择期手术,4 月 1 日开始进行常规基于实验室的 COVID-19 筛查。将围手术期检测到 COVID-19 的患者与对照组进行死亡率、并发症和入住重症监护病房(ICU)的比较。
在 468 例患者中,有 36 例(7.7%)确诊 COVID-19。在这些 COVID-19 患者中,55.6%在术前发现,44.4%在术后发现。在常规术前 COVID-19 实验室筛查之前,术前诊断的病例占 7.7%,而筛查后则占 65.2%(P=0.0008)。COVID-19 患者的围手术期死亡率为 16.7%,而 COVID-19 阴性患者为 1.4%[调整风险比(aRR)=9.29;95%置信区间(CI),5.68-15.21]。COVID-19 患者中严重并发症的发生率为 58.3%,而对照组为 6.0%(aRR=7.02;95%CI,4.96-9.92)。COVID-19 患者中更常见的是心脏骤停、脓毒症/休克、呼吸衰竭、肺炎、急性呼吸窘迫综合征和急性肾损伤。COVID-19 患者的 ICU 入住率为 36.1%,而对照组为 16.4%(aRR=1.34;95%CI,0.86-2.09)。
COVID-19 与严重围手术期发病率和死亡率的风险增加相关。大量 COVID-19 患者直到手术后才被发现。