Emory Healthcare (EHC) Office of Quality and Risk, EHC Telehealth Team, and Emory University School of Medicine Department of Neurology, Atlanta, Georgia.
EHC Telehealth Team.
J Healthc Manag. 2020 Nov-Dec;65(6):443-452. doi: 10.1097/JHM-D-20-00131.
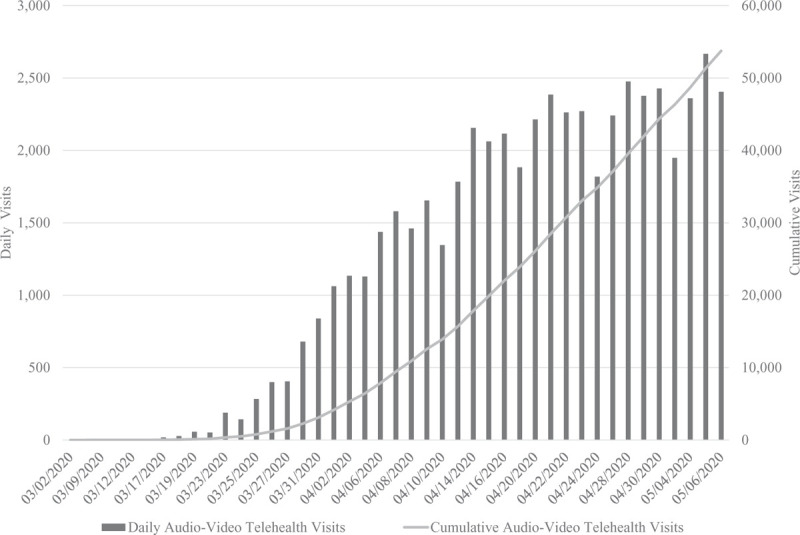
The COVID-19 pandemic, with its resultant social distancing, has disrupted the delivery of healthcare for both patients and providers. Fortunately, changes to legislation and regulation in response to the pandemic allowed Emory Healthcare to rapidly implement telehealth care. Beginning in early March 2020 and continuing through the initial 2-month implementation period (when data collection stopped), clinicians received telehealth training and certification. Standard workflows created by means of a hub-and-spoke operational model enabled rapid sharing and deployment of best practices throughout the system's physician group practice. Lean process huddles facilitated successful implementation. In total, 2,374 healthcare professionals, including 986 attending physicians, 416 residents and fellows, and 555 advanced practice providers, were trained and certified for telehealth; 53,751 new- and established-patient audio-video telehealth visits and 10,539 established-patient telephone visits were performed in 8 weeks for a total of 64,290 virtual visits. This initiative included a new COVID-19 virtual patient clinic that saw 705 patients in a 6-week period. A total of $14,662,967 was charged during this time; collection rates were similar to in-person visits. Initial patient satisfaction scores were equivalent to in-person visits. We conclude that rapid deployment of virtual visits can be accomplished through a structured, organized approach including training, certification, and Lean principles. A hub-and-spoke model enables bidirectional feedback and timely improvements, thus facilitating swifter implementation and a quick rise in patient volume. Financial sustainability is achievable, but to sustain that, telehealth requires the support of continued deregulation by legislative and regulatory bodies.
新冠疫情导致的社交隔离,扰乱了医患双方的医疗服务提供。幸运的是,立法和监管方面的变化,使得埃默里医疗保健系统能够迅速实施远程医疗。从 2020 年 3 月初开始,并持续到最初的 2 个月实施期(数据收集停止时),临床医生接受了远程医疗培训和认证。通过轮辐式运营模式创建的标准工作流程,使最佳实践能够在整个系统的医师集团实践中迅速共享和部署。精益流程会议促进了成功实施。总共有 2374 名医疗保健专业人员接受了远程医疗培训和认证,包括 986 名主治医生、416 名住院医师和研究员以及 555 名高级执业医师;在 8 周内共进行了 53751 次新患者和已建立患者的音频视频远程医疗访问和 10539 次已建立患者的电话访问,总共有 64290 次虚拟访问。这一举措包括一个新的新冠病毒虚拟患者诊所,在 6 周内接待了 705 名患者。在此期间共收取了 14662967 美元;收费率与面对面就诊相似。最初的患者满意度评分与面对面就诊相同。我们的结论是,通过培训、认证和精益原则等结构化、组织化的方法,可以实现虚拟就诊的快速部署。轮辐式模型可以实现双向反馈和及时改进,从而促进更快的实施和患者数量的快速增加。财务可持续性是可以实现的,但为了维持这种情况,远程医疗需要立法和监管机构继续放宽监管的支持。