Stollery Children's Hospital Edmonton Alberta Canada.
Kirklin Institute for Research in Surgical Outcomes University of Alabama at Birmingham AL.
J Am Heart Assoc. 2020 Nov 3;9(21):e011890. doi: 10.1161/JAHA.118.011890. Epub 2020 Oct 20.
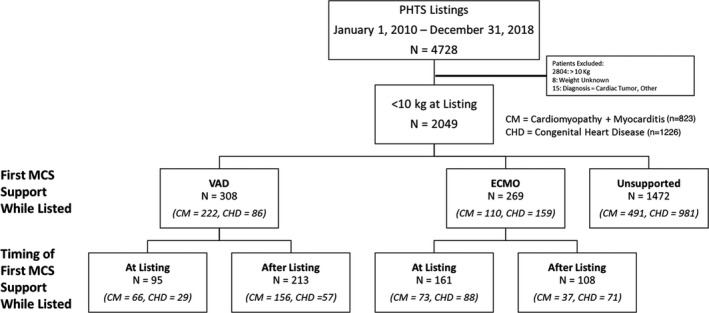
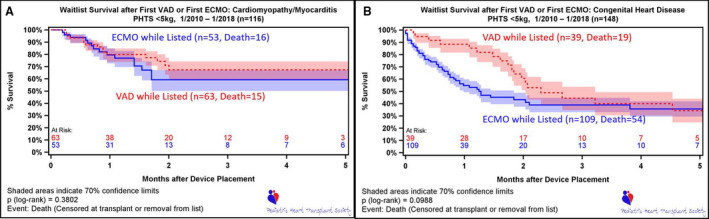
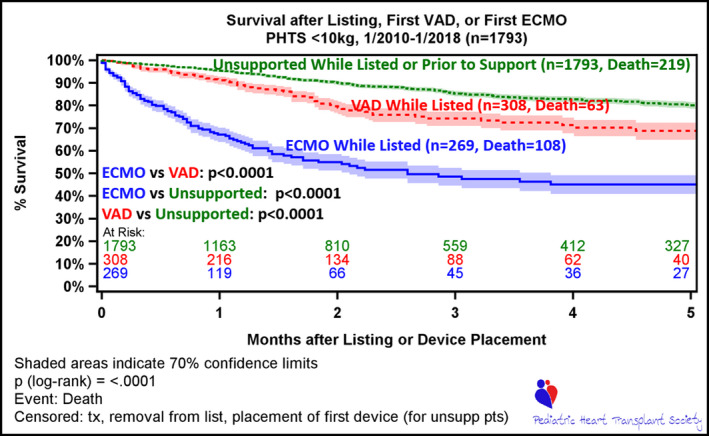
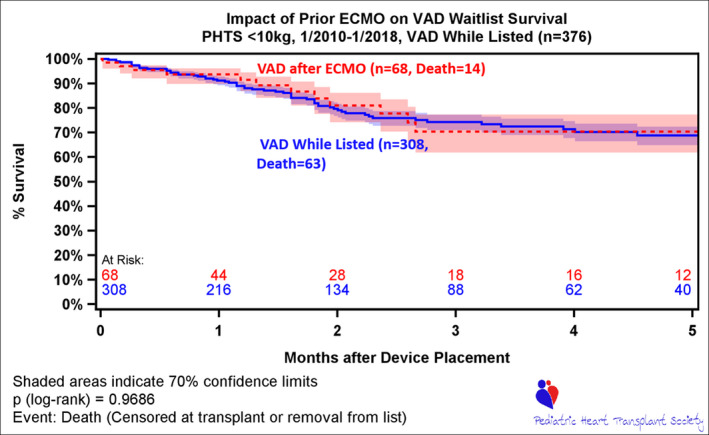
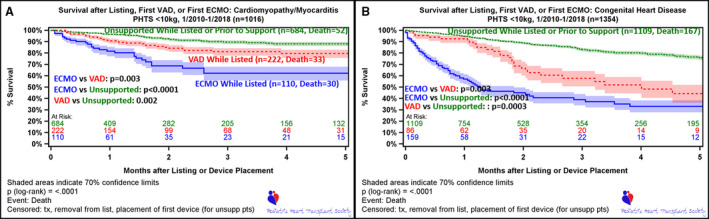
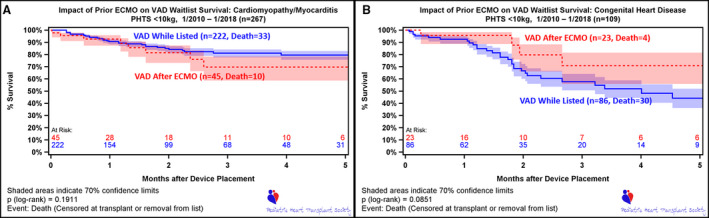
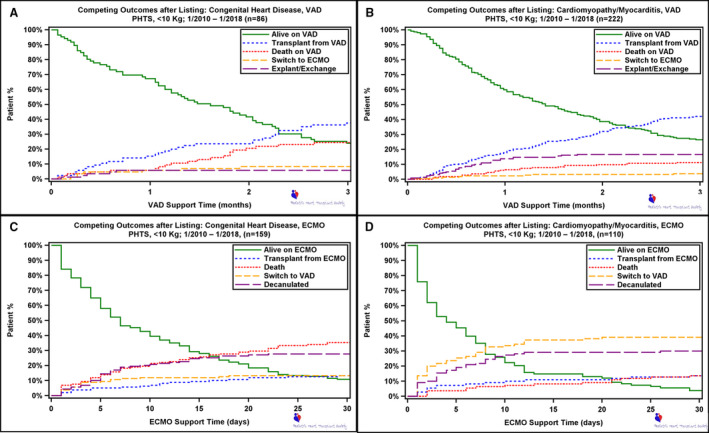
Background Infants with heart failure remain at significant risk for wait list mortality, despite mechanical circulatory support (MCS). It is unclear if the outcomes are influenced by modality of support or underlying diagnosis. We sought to compare the outcomes of infants <10 kg, focusing on modality of support and underlying diagnosis. Methods and Results Using the Pediatric Heart Transplant Society database, we evaluated survival following first MCS device in children <10 kg who were listed for heart transplant between 2010 and 2018. There were 2049 children <10 kg, with the predominant diagnosis being congenital heart disease (CHD) (59.8% [n=1226]) and 28.1% (n=577) requiring MCS. Extracorporeal membrane oxygenation (ECMO) was the most common form of MCS at listing, with ventricular assist device (VAD) more common after listing. There was no difference in the use of ECMO at or after listing for cardiomyopathy versus CHD (8.9% versus 7.2%; =0.2; 5.4% versus 6.4%; =0.4). However, there was a significant difference in the use of VAD both at listing (8% versus 2.4%; <0.001) and after (22.8% versus 5.1%; <0.001) between the 2 groups. When comparing these groups, patients with CHD were smaller and younger and had a higher proportion with previous cardiac surgery. Survival at 3 months demonstrated better survival for VAD therapy compared with ECMO (74.3% versus 48.6%; <0.001). In patients <5 kg, survival did not differ between ECMO and VAD (=0.01) for the CHD or the cardiomyopathy group (=0.38), but patients with cardiomyopathy demonstrated better survival on both forms of support. Conclusions Survival for patients <10 kg on ECMO is inferior compared with VAD. Patients with cardiomyopathy <5 kg had better survival with both modes of MCS compared with those with CHD. These findings support the need for small, durable devices for neonates and infants, with particular focus in patients with CHD.
背景
尽管有机械循环支持(MCS),心力衰竭的婴儿在等待名单上仍然面临着很高的死亡率。目前尚不清楚这些结果是否受到支持方式或潜在诊断的影响。我们旨在比较 10 公斤以下婴儿的结局,重点关注支持方式和潜在诊断。
方法和结果
使用儿科心脏移植协会数据库,我们评估了 2010 年至 2018 年期间在等待心脏移植的 10 公斤以下儿童中首次 MCS 设备后的生存情况。共有 2049 名 10 公斤以下的儿童,主要诊断为先天性心脏病(CHD)(59.8%[n=1226])和 28.1%(n=577)需要 MCS。体外膜氧合(ECMO)是列入名单时最常见的 MCS 形式,而心室辅助装置(VAD)在列入名单后更为常见。在心肌病与 CHD 患者中,列入名单时或列入名单后的 ECMO 使用无差异(8.9%对 7.2%;=0.2;5.4%对 6.4%;=0.4)。然而,两组之间在列入名单时(8%对 2.4%;<0.001)和列入名单后(22.8%对 5.1%;<0.001)VAD 的使用有显著差异。在比较这些组时,CHD 患者的体型较小,年龄较小,且既往心脏手术比例较高。3 个月的生存率显示 VAD 治疗的生存率优于 ECMO(74.3%对 48.6%;<0.001)。在<5 公斤的患者中,ECMO 与 VAD 之间的生存率在 CHD 或心肌病组之间没有差异(=0.01),但心肌病患者在两种支持方式下的生存率都更好。
结论
与 VAD 相比,ECMO 支持的<10 公斤患儿的生存率较低。与 CHD 患者相比,<5 公斤的心肌病患者使用两种 MCS 模式的生存率更高。这些发现支持为新生儿和婴儿提供小型、耐用的设备,特别是在 CHD 患者中。