Fundació Sida i Societat, Technical Advisor Unit (UAT), Escuintla National Hospital, Escuintla, 5001, Guatemala.
Population Health Program, Tuberculosis Group, Texas Biomedical Research Institute, San Antonio, TX, 78227, USA.
AIDS Res Ther. 2020 Oct 19;17(1):62. doi: 10.1186/s12981-020-00318-8.
Improved point-of-care diagnostic tests for tuberculosis (TB) in severe immune suppressed people living with HIV (PLWH) are needed to decrease morbidity and mortality outcomes. The aim of the study is to evaluate the performance of the lipoarabinomannan antigen test (LAM-test) with and without α-mannosidase pre-treated urine in a cohort of PLWH in primary care clinics in Guatemala. We further determined TB incidence, and mortality rates and its risk factors in PLWH with TB symptoms.
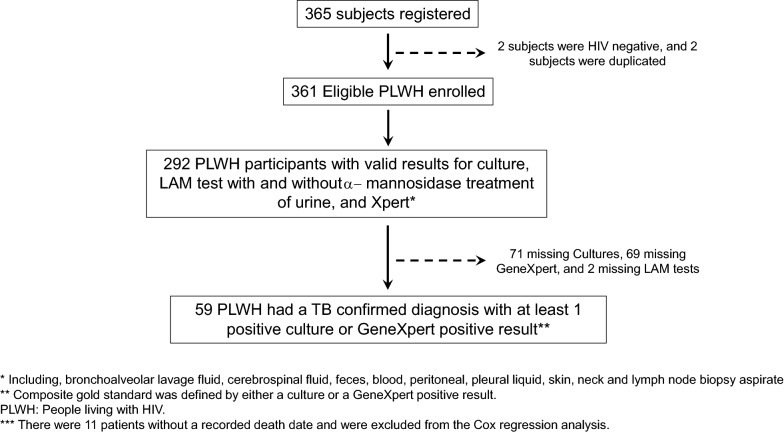
Prospective longitudinal study of PLWH with TB symptoms. Urine samples were collected at 2 HIV sites to test the sensitivity of the LAM-test in urine with and without α-mannosidase pre-treatment. A composite reference standard of either a positive Mycobacterium tuberculosis complex culture and/or GeneXpert MTB/RIF (Xpert, Cepheid, Sunnyvale, CA, USA) results was used in the LAM-test diagnostic accuracy studies. Cox proportional hazards regression was used to study mortality predictors.
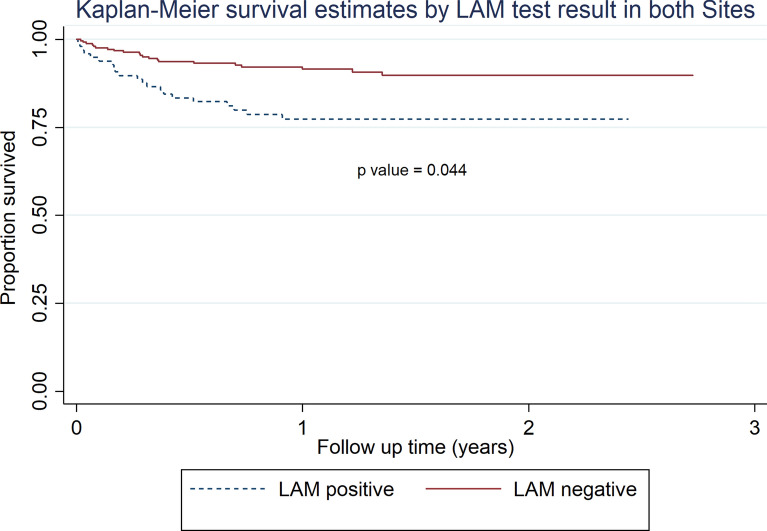
The overall sensitivity of the LAM-test was of 56.1% with 95% CI of (43.3-68.3). There were no differences in the LAM-test sensitivity neither by hospital nor by CD4 T cell values. LAM-test sensitivity in PLWH with < 200 CD4 T cells/µl was of 62.2% (95% CI 46.5-76.2). There were no significant differences in sensitivity when comparing LAM-test results obtained from untreated vs. α-mannosidase treated urine [55.2% (95% CI 42.6-67.4) vs. 56.9% (95% CI 44-69.2), respectively]. TB incidence in our cohort was of 21.4/100 person years (PYs) (95% CI 16.6-27.6), and mortality rate was of 11.1/100 PYs (95% CI 8.2-15.0). Importantly, PLWH with a positive LAM-test result had an adjusted hazard ratio (aHR) of death of 1.98 (1.0-3.8) with a significant p value of 0.044 when compared to PLWH with a negative LAM-test result.
In this study, α-mannosidase treatment of urine did not significantly increase the LAM-test performance, however; this needs to be further evaluated in a large-scale study due to our study limitations. Importantly, high rates of TB incidence and mortality were found, and a positive LAM-test result predicted mortality in PLWH with TB clinical symptoms.
需要改进针对严重免疫抑制的艾滋病毒感染者(PLWH)的结核病(TB)即时检测,以降低发病率和死亡率。本研究的目的是评估脂阿拉伯甘露聚糖抗原检测(LAM 检测)及其经α-甘露糖苷酶预处理尿液在危地马拉初级保健诊所 PLWH 队列中的性能。我们还确定了 PLWH 出现 TB 症状后的 TB 发生率、死亡率及其危险因素。
对有 TB 症状的 PLWH 进行前瞻性纵向研究。在 2 个 HIV 检测点采集尿液样本,以检测未经α-甘露糖苷酶预处理和预处理尿液中 LAM 检测的敏感性。LAM 检测的诊断准确性研究采用结核分枝杆菌复合体培养阳性和/或 GeneXpert MTB/RIF(Xpert,Cepheid,Sunnyvale,CA,USA)结果的复合参考标准。使用 Cox 比例风险回归研究死亡率预测因素。
LAM 检测的总敏感性为 56.1%(95%CI 43.3-68.3)。医院和 CD4 T 细胞值对 LAM 检测的敏感性没有差异。CD4 T 细胞/µl<200 的 PLWH 的 LAM 检测敏感性为 62.2%(95%CI 46.5-76.2)。比较未经处理的尿液和经α-甘露糖苷酶处理的尿液中 LAM 检测结果的敏感性时,差异无统计学意义[分别为 55.2%(95%CI 42.6-67.4)和 56.9%(95%CI 44-69.2)]。本队列的 TB 发病率为 21.4/100 人年(95%CI 16.6-27.6),死亡率为 11.1/100 人年(95%CI 8.2-15.0)。重要的是,与 LAM 检测结果阴性的 PLWH 相比,LAM 检测结果阳性的 PLWH 的死亡调整风险比(aHR)为 1.98(1.0-3.8),具有显著的 p 值 0.044。
在这项研究中,尿液的α-甘露糖苷酶处理并没有显著提高 LAM 检测的性能,但由于研究的局限性,这需要在一项大规模研究中进一步评估。重要的是,我们发现 TB 的发病率和死亡率很高,TB 临床症状阳性的 PLWH 的 LAM 检测结果预测死亡率。