Hospital for Special Surgery.
Weill Cornell Medical College, New York, NY, USA.
Spine (Phila Pa 1976). 2021 Feb 1;46(3):E203-E212. doi: 10.1097/BRS.0000000000003751.
A retrospective cohort study.
The aim of this study was to identify an association between preoperative opioid use and reoperations rates.
Chronic opioid use is a public health crisis in the United States and has been linked to worse outcomes after lumbar spine surgery. However, no studies have identified an association between preoperative opioid use and reoperations rates.
A retrospective cohort study was conducted using patients from one private insurance database who underwent primary lumbar decompression/discectomy (LDD) or posterior/transforaminal lumbar interbody fusion (PLIF/TLIF). Preoperative use of five specific opioid medications (tramadol, hydromorphone, oxycodone, hydromorphone, and extended-release oxycodone) was categorized as acute (within 3 months), subacute (acute use and use between 3 and 6 months), or chronic (subacute use and use before 6 months). Multivariate regression, controlling for multilevel surgery, age, sex, and Charlson Comorbidity Index, was used to determine the association of each medication on reoperations within 5 years.
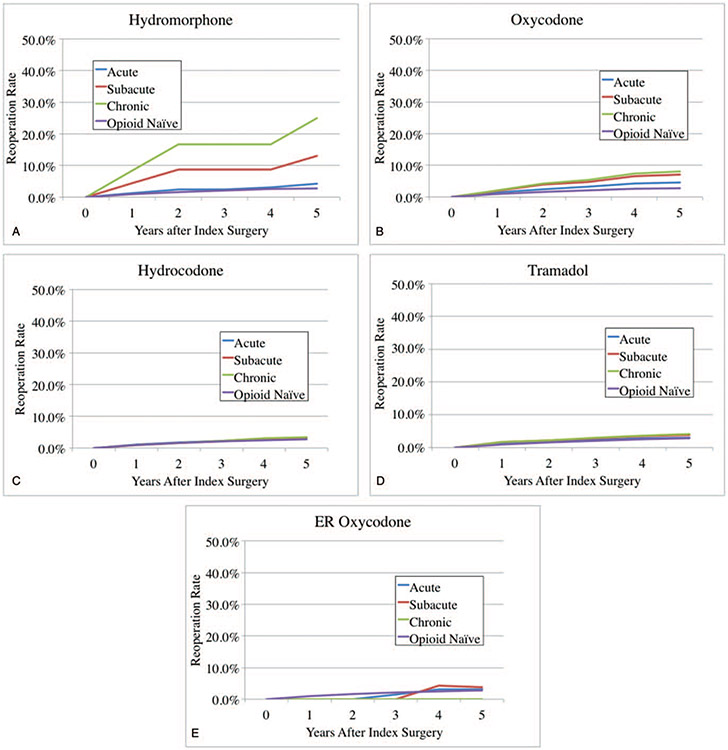
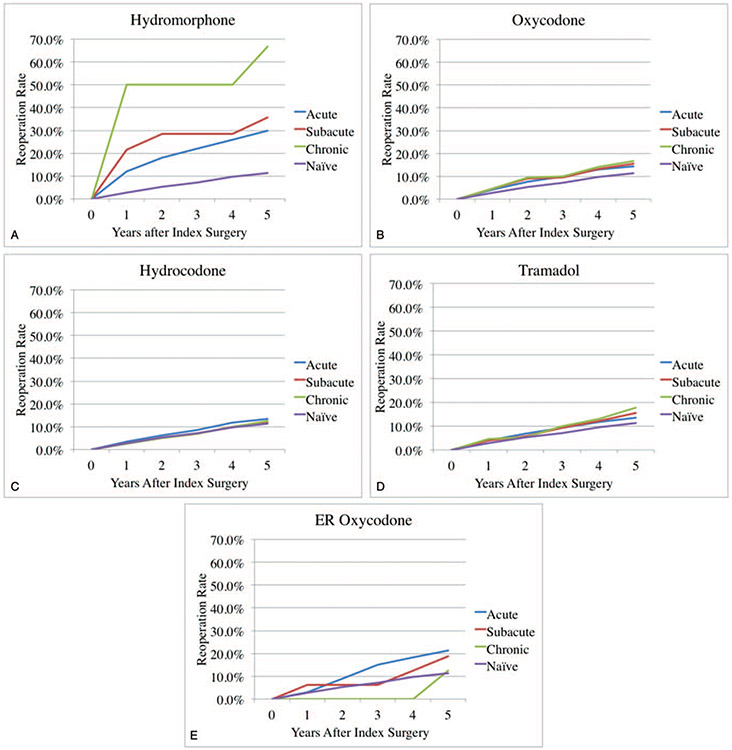
A total of 11,551 patients undergoing LDD and 3291 patients undergoing PLIF/TLIF without previous lumbar spine surgery were identified. In the LDD group, opioid-naïve patients had a 5-year reoperation rate of 2.8%, compared with 25.0% and 8.0 with chronic preoperative use of hydromorphone and oxycodone, respectively. In multivariate analysis, any preoperative use of oxycodone was associated with increased reoperations (odds ratios [OR] = 1.4, 2.0, and 2.3, for acute, subacute, and chronic use; P < 0.01). Chronic use of hydromorphone was also associated with increased reoperations (OR = 7.5, P < 0.01).In the PLIF/TLIF group, opioid-naïve patients had a 5-year reoperation rate of 11.3%, compared with 66.7% and 16.8% with chronic preoperative use of hydromorphone and oxycodone, respectively. In multivariate analysis, any preoperative use of hydromorphone was associated with increased reoperations (OR = 2.9, 4.0, and 14.0, for acute, subacute, and chronic use; P < 0.05).
Preoperative use of the higher-potency opioid medications is associated with increased reoperations after LDD and PLIF/TLIF in a dose-dependent manner. Surgeons should use this data for preoperative opioid cessation counseling and individualized risk stratification.Level of Evidence: 3.
回顾性队列研究。
本研究旨在确定术前使用阿片类药物与再次手术率之间的关联。
慢性阿片类药物使用在美国是一个公共健康危机,与腰椎手术后的预后较差有关。然而,尚无研究确定术前使用阿片类药物与再次手术率之间的关联。
使用来自一个私人保险数据库的接受初次腰椎减压/椎间盘切除术(LDD)或后路/经椎间孔腰椎体间融合术(PLIF/TLIF)的患者进行回顾性队列研究。将五种特定阿片类药物(曲马多、氢吗啡酮、羟考酮、氢吗啡酮和羟考酮缓释剂)的术前使用分为急性(3 个月内)、亚急性(急性使用和 3 至 6 个月之间使用)或慢性(亚急性使用和 6 个月前使用)。使用多变量回归,控制多层次手术、年龄、性别和 Charlson 合并症指数,以确定每种药物在 5 年内再次手术的相关性。
共确定了 11551 例接受 LDD 和 3291 例接受无先前腰椎手术的 PLIF/TLIF 的患者。在 LDD 组中,阿片类药物无使用史的患者 5 年再次手术率为 2.8%,而慢性术前使用氢吗啡酮和羟考酮的患者分别为 25.0%和 8.0%。在多变量分析中,任何术前使用羟考酮均与增加再次手术相关(优势比[OR]分别为 1.4、2.0 和 2.3,用于急性、亚急性和慢性使用;P<0.01)。慢性使用氢吗啡酮也与增加再次手术相关(OR=7.5,P<0.01)。在 PLIF/TLIF 组中,阿片类药物无使用史的患者 5 年再次手术率为 11.3%,而慢性术前使用氢吗啡酮和羟考酮的患者分别为 66.7%和 16.8%。在多变量分析中,任何术前使用氢吗啡酮均与增加再次手术相关(OR 分别为 2.9、4.0 和 14.0,用于急性、亚急性和慢性使用;P<0.05)。
术前使用更高效的阿片类药物与 LDD 和 PLIF/TLIF 后的再次手术呈剂量依赖性相关。外科医生应使用这些数据进行术前阿片类药物戒断咨询和个体化风险分层。
3 级。