Department of Population Health, Luxembourg Institute of Health, Strassen, Luxembourg.
Department of Family Medicine, Care and Public Health Research Institute, Maastricht University, Maastricht, The Netherlands.
PLoS One. 2020 Oct 20;15(10):e0240024. doi: 10.1371/journal.pone.0240024. eCollection 2020.
An increasing number of diseases is linked to deterioration of quality of life (QoL). Part of this association can be explained by socio-economic factors, which are most commonly accounted for. Our aim was to explore the potential contribution of other factors related to clinical burden, social interaction and functioning.
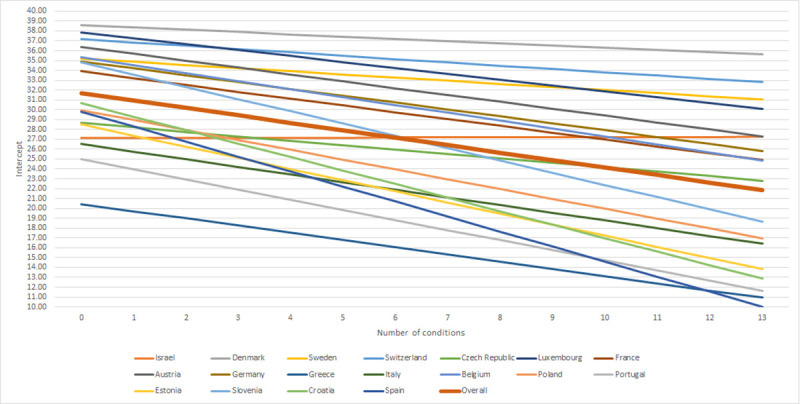
A cross-sectional analysis was conducted on wave 6 of the population-based Survey of Health, Ageing and Retirement in Europe (SHARE), among participants aged 50+ (n = 67 179). The Control, Autonomy, Self-Realization and Pleasure (CASP-12v1) questionnaire measured QoL. The association between number of diseases and QoL was tested in a mixed-effects linear regression model. The base model controlled for socio-economic characteristics. Factors of interest (symptoms, polypharmacy, unmet care needs, utilisation of care, social network, personal and financial help, loneliness and activities of daily living (ADL) with instrumental activities (IADL)) were added to the base model one at a time and tested for relevance (i.e. change in the β-coefficient of the number of conditions of 15% or more).
Symptoms, polypharmacy, loneliness and ADL/IADL appeared relevant and were retained in the final model. The association between number of conditions and QoL in the base model was -2.44 [95% CI: -2.72; -2.16], while this association was -0.76 [95%CI: -0.97; -0.54] after all relevant factors were included.
Factors beyond the socio-economic circumstances play an important role in explaining the association between number of conditions and QoL. These factors should be considered to better estimate the impact of chronic diseases on QoL, and for improving patient care.
越来越多的疾病与生活质量(QoL)下降有关。这种关联的一部分可以用社会经济因素来解释,这些因素是最常见的解释因素。我们的目的是探讨与临床负担、社会互动和功能相关的其他因素的潜在贡献。
对基于人群的欧洲老龄化与退休研究第六波(SHARE)中 50 岁及以上的参与者(n=67179)进行了横断面分析。控制、自主、自我实现和快乐(CASP-12v1)问卷测量了 QoL。在混合效应线性回归模型中测试了疾病数量与 QoL 之间的关联。基础模型控制了社会经济特征。逐个向基础模型中添加感兴趣的因素(症状、多种药物治疗、未满足的护理需求、护理利用、社交网络、个人和财务帮助、孤独感和日常生活活动(ADL)与工具性日常生活活动(IADL)),并测试其相关性(即条件数量的β系数变化 15%或更多)。
症状、多种药物治疗、孤独感和 ADL/IADL 似乎相关,并保留在最终模型中。基础模型中疾病数量与 QoL 的关联为-2.44[95%CI:-2.72;-2.16],而纳入所有相关因素后,该关联为-0.76[95%CI:-0.97;-0.54]。
社会经济环境以外的因素在解释疾病数量与 QoL 之间的关联方面起着重要作用。这些因素应被考虑在内,以更好地估计慢性疾病对 QoL 的影响,并改善患者护理。