Baylor Heart and Vascular Institute, Baylor University Medical Center, Dallas, TX (M.P.).
Imperial College, London, UK (M.P.).
Circulation. 2021 Jan 26;143(4):326-336. doi: 10.1161/CIRCULATIONAHA.120.051783. Epub 2020 Oct 21.
Empagliflozin reduces the risk of cardiovascular death or hospitalization for heart failure in patients with heart failure and a reduced ejection fraction, with or without diabetes, but additional data are needed about the effect of the drug on inpatient and outpatient events that reflect worsening heart failure.
We randomly assigned 3730 patients with class II to IV heart failure with an ejection fraction of ≤40% to double-blind treatment with placebo or empagliflozin (10 mg once daily), in addition to recommended treatments for heart failure, for a median of 16 months. We prospectively collected information on inpatient and outpatient events reflecting worsening heart failure and prespecified their analysis in individual and composite end points.
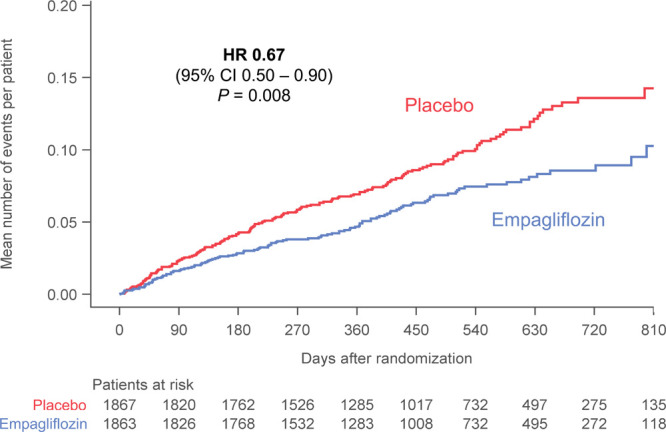
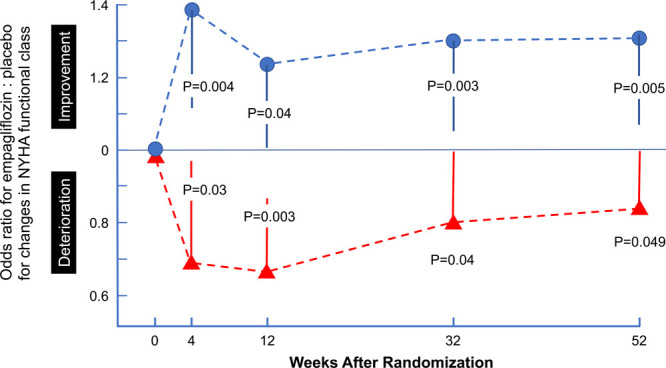
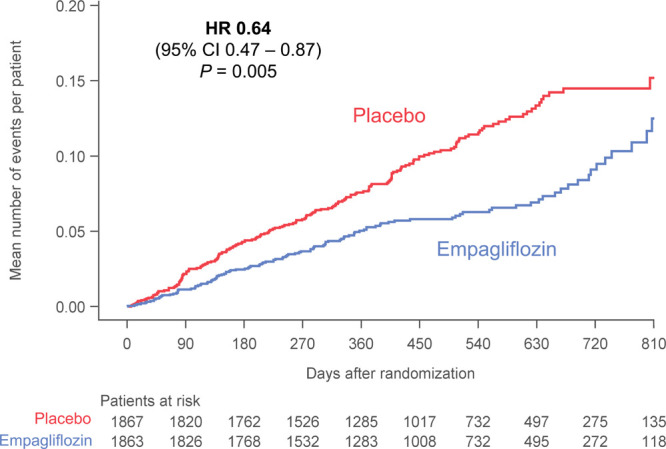
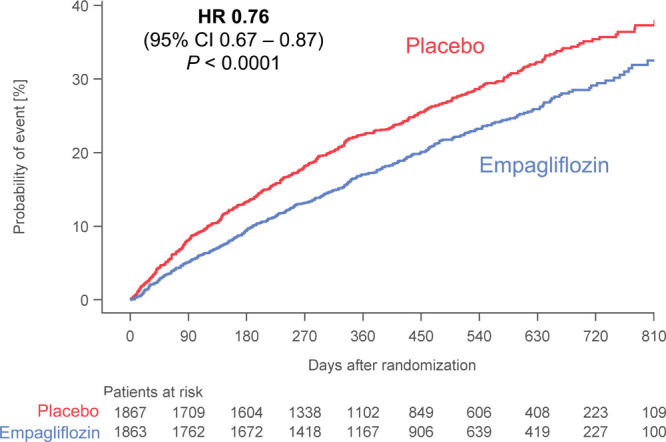
Empagliflozin reduced the combined risk of death, hospitalization for heart failure or an emergent/urgent heart failure visit requiring intravenous treatment (415 versus 519 patients; empagliflozin versus placebo, respectively; hazard ratio [HR], 0.76; 95% CI, 0.67-0.87; <0.0001). This benefit reached statistical significance at 12 days after randomization. Empagliflozin reduced the total number of heart failure hospitalizations that required intensive care (HR, 0.67; 95% CI, 0.50-0.90; =0.008) and that required a vasopressor or positive inotropic drug or mechanical or surgical intervention (HR, 0.64; 95% CI, 0.47-0.87; =0.005). As compared with placebo, fewer patients in the empagliflozin group reported intensification of diuretics (297 versus 414 [HR, 0.67; 95% CI, 0.56-0.78; <0.0001]). Additionally, patients assigned to empagliflozin were 20% to 40% more likely to experience an improvement in New York Heart Association functional class and were 20% to 40% less likely to experience worsening of New York Heart Association functional class, with statistically significant effects that were apparent 28 days after randomization and maintained during long-term follow-up. The risk of any inpatient or outpatient worsening heart failure event in the placebo group was high (48.1 per 100 patient-years of follow-up), and it was reduced by empagliflozin (HR, 0.70; 95% CI, 0.63-0.78; <0.0001).
In patients with heart failure and a reduced ejection fraction, empagliflozin reduced the risk and total number of inpatient and outpatient worsening heart failure events, with benefits seen early after initiation of treatment and sustained for the duration of double-blind therapy. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03057977.
恩格列净可降低射血分数降低的心力衰竭患者(无论是否合并糖尿病)的心血管死亡或心力衰竭住院风险,但仍需要更多关于该药对反映心力衰竭恶化的住院和门诊事件影响的数据。
我们将 3730 名射血分数≤40%的 II 级至 IV 级心力衰竭患者随机分组,接受安慰剂或恩格列净(每日 10mg,一次)的双盲治疗,此外还接受心力衰竭的推荐治疗,中位随访时间为 16 个月。我们前瞻性地收集了反映心力衰竭恶化的住院和门诊事件信息,并预先设定了个体和综合终点的分析。
恩格列净降低了死亡、心力衰竭住院或因心力衰竭恶化需要静脉治疗的紧急/紧急心力衰竭就诊的复合风险(分别为 415 例和 519 例;恩格列净与安慰剂相比,风险比[HR]为 0.76;95%置信区间[CI]为 0.67-0.87;<0.0001)。这种益处在随机分组后 12 天达到统计学意义。恩格列净降低了需要重症监护的心力衰竭住院总数(HR,0.67;95%CI,0.50-0.90;=0.008)和需要血管加压素或正性肌力药物或机械或手术干预的心力衰竭住院(HR,0.64;95%CI,0.47-0.87;=0.005)。与安慰剂相比,恩格列净组报告利尿剂强化治疗的患者(297 例与 414 例[HR,0.67;95%CI,0.56-0.78;<0.0001])更少。此外,接受恩格列净治疗的患者纽约心脏协会(NYHA)心功能分级改善的可能性增加 20%至 40%,NYHA 心功能分级恶化的可能性降低 20%至 40%,且在随机分组后 28 天即可观察到有统计学意义的效果,并在长期随访中持续存在。安慰剂组任何住院或门诊心力衰竭恶化事件的风险均较高(每 100 患者年随访 48.1 例),恩格列净可降低该风险(HR,0.70;95%CI,0.63-0.78;<0.0001)。
在射血分数降低的心力衰竭患者中,恩格列净降低了住院和门诊心力衰竭恶化事件的风险和总数,治疗开始后早期即有获益,并在双盲治疗期间持续获益。