Clinical Trial Unit, Istituto Nazionale Tumori, IRCCS, Fondazione G. Pascale, Napoli, Italy.
Melanoma, Cancer Immunotherapy and Development Therapeutics Unit, Istituto Nazionale Tumori, IRCCS, Fondazione G. Pascale, Napoli, Italy.
J Transl Med. 2020 Oct 21;18(1):405. doi: 10.1186/s12967-020-02573-9.
Tocilizumab blocks pro-inflammatory activity of interleukin-6 (IL-6), involved in pathogenesis of pneumonia the most frequent cause of death in COVID-19 patients.
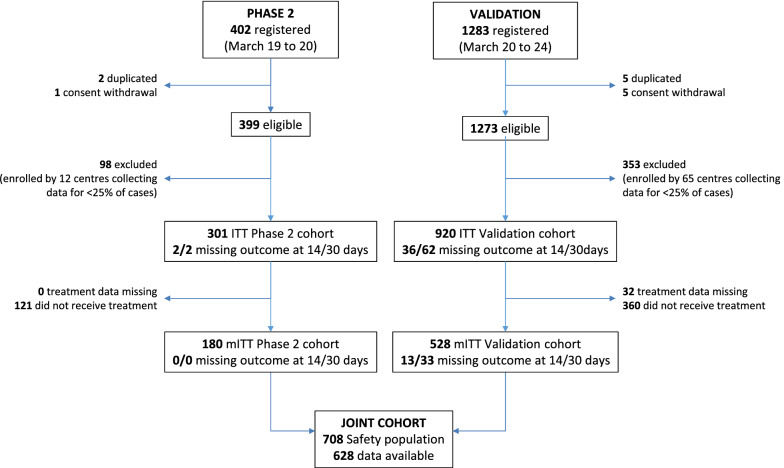
A multicenter, single-arm, hypothesis-driven trial was planned, according to a phase 2 design, to study the effect of tocilizumab on lethality rates at 14 and 30 days (co-primary endpoints, a priori expected rates being 20 and 35%, respectively). A further prospective cohort of patients, consecutively enrolled after the first cohort was accomplished, was used as a secondary validation dataset. The two cohorts were evaluated jointly in an exploratory multivariable logistic regression model to assess prognostic variables on survival.
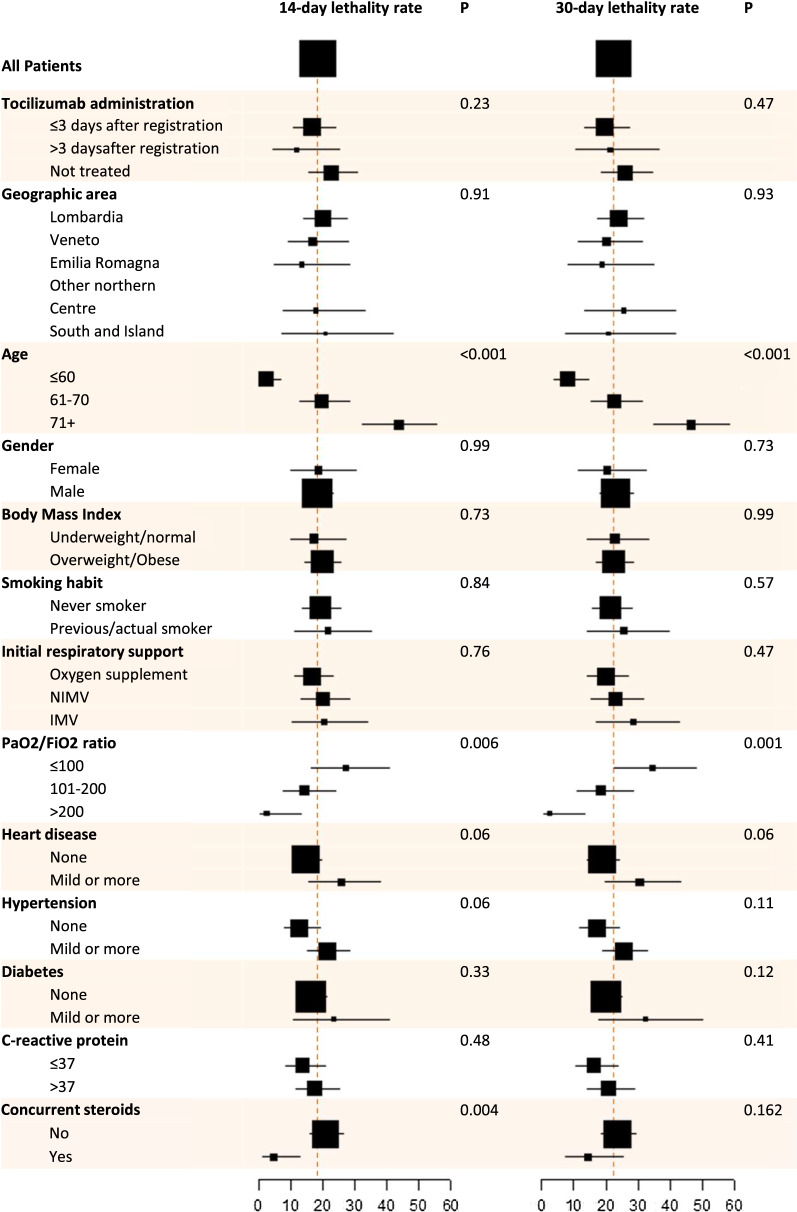
In the primary intention-to-treat (ITT) phase 2 population, 180/301 (59.8%) subjects received tocilizumab, and 67 deaths were observed overall. Lethality rates were equal to 18.4% (97.5% CI: 13.6-24.0, P = 0.52) and 22.4% (97.5% CI: 17.2-28.3, P < 0.001) at 14 and 30 days, respectively. Lethality rates were lower in the validation dataset, that included 920 patients. No signal of specific drug toxicity was reported. In the exploratory multivariable logistic regression analysis, older age and lower PaO2/FiO2 ratio negatively affected survival, while the concurrent use of steroids was associated with greater survival. A statistically significant interaction was found between tocilizumab and respiratory support, suggesting that tocilizumab might be more effective in patients not requiring mechanical respiratory support at baseline.
Tocilizumab reduced lethality rate at 30 days compared with null hypothesis, without significant toxicity. Possibly, this effect could be limited to patients not requiring mechanical respiratory support at baseline. Registration EudraCT (2020-001110-38); clinicaltrials.gov (NCT04317092).
托珠单抗阻断白细胞介素-6(IL-6)的促炎活性,IL-6 与 COVID-19 患者最常见的死亡原因肺炎的发病机制有关。
根据 2 期设计,计划进行一项多中心、单臂、假设驱动的试验,以研究托珠单抗对 14 天和 30 天死亡率的影响(主要终点,预期预先设定的死亡率分别为 20%和 35%)。在第一队列完成后,连续招募的进一步前瞻性队列患者被用作二次验证数据集。两个队列在探索性多变量逻辑回归模型中联合评估,以评估生存的预后变量。
在主要意向治疗(ITT)2 期人群中,180/301(59.8%)名患者接受了托珠单抗治疗,总共有 67 例死亡。14 天和 30 天的死亡率分别为 18.4%(97.5%CI:13.6-24.0,P=0.52)和 22.4%(97.5%CI:17.2-28.3,P<0.001)。验证数据集中的死亡率较低,该数据集包括 920 名患者。未报告特定药物毒性的信号。在探索性多变量逻辑回归分析中,年龄较大和较低的 PaO2/FiO2 比值与生存率降低相关,而同时使用类固醇与生存率增加相关。托珠单抗和呼吸支持之间存在统计学显著的交互作用,表明托珠单抗可能对基线时不需要机械呼吸支持的患者更有效。
与零假设相比,托珠单抗降低了 30 天的死亡率,且没有显著毒性。可能,这种效果仅限于基线时不需要机械呼吸支持的患者。登记号 EudraCT(2020-001110-38);临床试验.gov(NCT04317092)。