Department of Neurosurgery, Kyoto University Graduate School of Medicine.
Department of Otolaryngology, Head and Neck Surgery, Kyoto University Graduate School of Medicine.
Neurol Med Chir (Tokyo). 2020 Nov 15;60(11):553-562. doi: 10.2176/nmc.oa.2020-0060. Epub 2020 Oct 21.
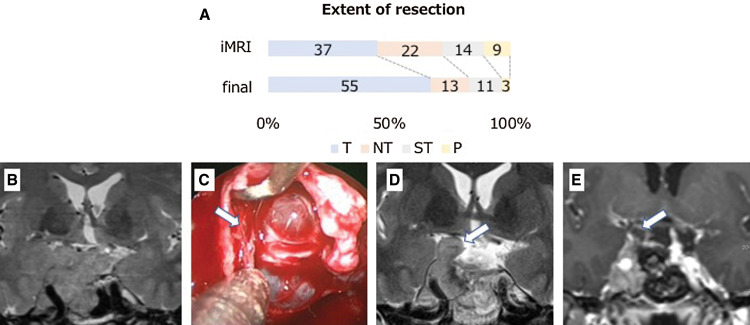
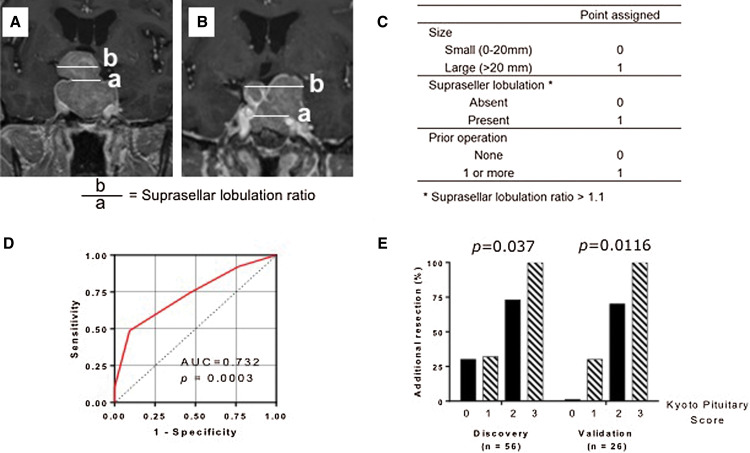
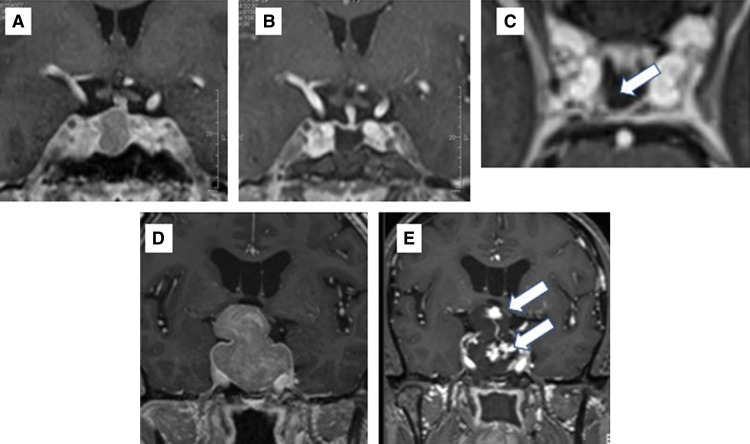
The aim of this study was to evaluate the impact of 3-Tesla intraoperative high-field magnetic resonance imaging (3T-iMRI) for pituitary adenoma resection, and to propose a new scoring system for predicting the utility of 3T-iMRI. This retrospective study evaluated 82 patients with pituitary adenoma who underwent purely endoscopic endonasal resection with 3T-iMRI between 2015 and 2019. 3T-iMRI revealed unexpected residual tumor in 39 cases (47.6%), which led to further resection and contributed to upgrading of the resection level in 28 cases (34.1%), which led to gross total resection rates (GTRs) of 67.1% and near total resection of 15.9%. To construct a new scoring system, patients were divided into a discovery cohort (56 patients) and a validation cohort (26 patients). Three variables for the scoring system were selected according to a univariate analysis of the discovery cohort: the size of the tumor (>20 mm: 1 point), the presence of suprasellar tumor lobulation (1 point) and the history of previous operations (1 point). The risk of additional resection after iMRI was well stratified by this scoring system (range 0-3; p = 0.0037 for trend). Robustness of the system was confirmed in the validation cohort (0 points, 0%; 1 point, 30.8%; 2 points, 70.0%; 3 points, 100%; p = 0.0116 for trend). These results indicate that 3T-iMRI optimized the extent of resection, even with the use of an endoscope, and that the proposed scoring system is useful for predicting whether 3T-iMRI is likely to be of value for a particular patient.
本研究旨在评估 3T 术中高场强磁共振成像(3T-iMRI)在垂体腺瘤切除中的作用,并提出一种新的评分系统来预测 3T-iMRI 的应用价值。本回顾性研究评估了 2015 年至 2019 年间 82 例接受 3T-iMRI 辅助内镜经鼻蝶入路垂体腺瘤切除术的患者。3T-iMRI 显示 39 例(47.6%)存在意外残留肿瘤,进一步切除后,28 例(34.1%)肿瘤切除程度升级,全切率(GTR)为 67.1%,近全切率为 15.9%。为构建新的评分系统,将患者分为发现队列(56 例)和验证队列(26 例)。根据发现队列的单因素分析,选择了评分系统的三个变量:肿瘤大小(>20mm:1 分)、鞍上肿瘤分叶存在(1 分)和既往手术史(1 分)。该评分系统很好地分层了 iMRI 后再次切除的风险(范围 0-3;趋势 p = 0.0037)。该系统在验证队列中得到了验证(0 分,0%;1 分,30.8%;2 分,70.0%;3 分,100%;趋势 p = 0.0116)。这些结果表明,3T-iMRI 优化了切除范围,即使使用内镜也是如此,且所提出的评分系统有助于预测 3T-iMRI 是否对特定患者有价值。