Godara Amandeep, Migliozzi Daniel R, Pilichowska Monika, Goyal Nitender, Varga Cindy, Gordon Craig E
Department of Hematology-Oncology, Tufts Medical Center, Boston, MA.
Kidney Transplant Team, Division of Nephrology, Tufts Medical Center, Boston, MA.
Kidney Med. 2020 Aug 5;2(5):652-656. doi: 10.1016/j.xkme.2020.06.007. eCollection 2020 Sep-Oct.
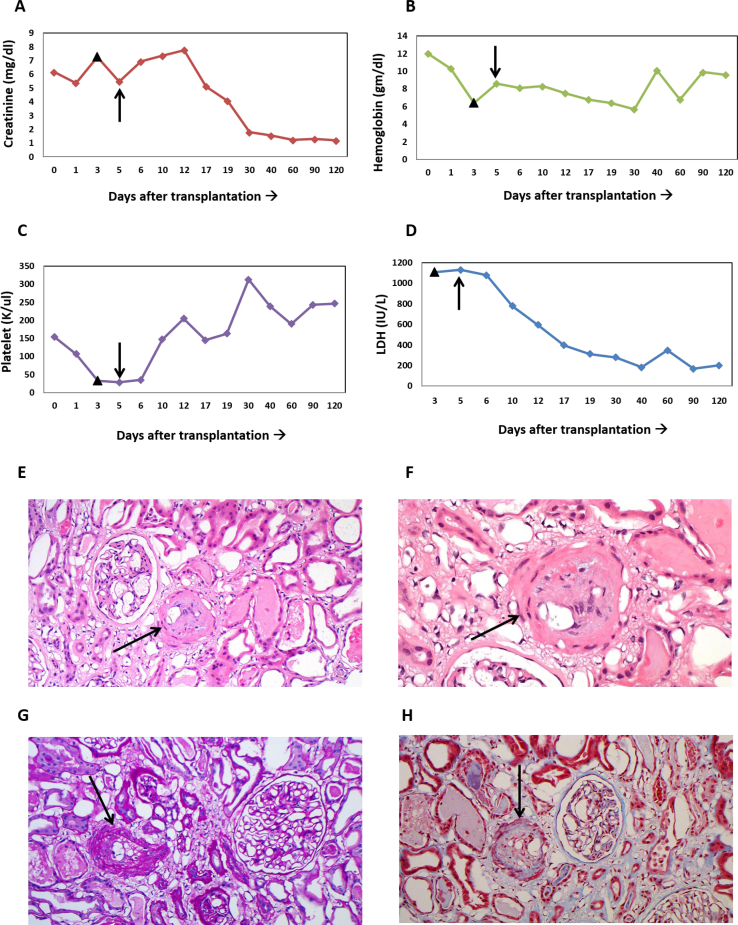
Transplant-associated thrombotic microangiopathy (TMA) in the post-organ transplantation setting occurs from a number of potential inciting factors, such as the use of calcineurin inhibitors, ischemic injury, infections, or antibody-mediated rejection leading to unchecked complement activation and end-organ damage. Delayed recognition of this condition can result in allograft loss. In this case description, we describe the first case of de novo TMA in a patient with polycystic kidney disease that occurred immediately after kidney transplantation. The diagnosis was made promptly on the basis of clinical and laboratory characteristics by a multidisciplinary team and confirmed through kidney biopsy, which showed acute TMA. The patient was successfully managed by replacing tacrolimus with belatacept, which targets cytotoxic T lymphocyte antigen 4, and use of eculizumab, a C5 inhibitor. Eculizumab treatment was discontinued after 3 months of complement inhibition on the patient's request, and relapse of TMA has not been encountered after more than 1 year of follow-up.
器官移植后发生的移植相关血栓性微血管病(TMA)由多种潜在诱发因素引起,如使用钙调神经磷酸酶抑制剂、缺血性损伤、感染或抗体介导的排斥反应,导致补体激活失控和终末器官损伤。对这种情况的延迟识别可能导致移植肾丢失。在本病例描述中,我们描述了一例多囊肾病患者肾移植后立即发生的新发TMA的首例病例。多学科团队根据临床和实验室特征迅速做出诊断,并通过肾活检得以证实,肾活检显示为急性TMA。通过将他克莫司替换为靶向细胞毒性T淋巴细胞抗原4的贝拉西普,并使用C5抑制剂依库珠单抗,成功治疗了该患者。应患者要求,在补体抑制3个月后停用依库珠单抗治疗,随访1年多后未出现TMA复发。