Department of Hepatobiliary Surgery, Xiangya Hospital, Central South University, Changsha, Hunan, China.
World J Surg Oncol. 2020 Oct 23;18(1):272. doi: 10.1186/s12957-020-02053-w.
Intrahepatic cholangiocarcinoma (ICC) stands as the second most common malignant tumor in the liver with poor patient prognosis. Increasing evidences have shown that inflammation plays a significant role in tumor progression, angiogenesis, and metastasis. However, the prognosis significance of inflammatory biomarkers on recurrence-free survival (RFS) and overall survival (OS) in ICC patients is poorly recognized.
ICC patients who underwent curative hepatectomy and diagnosed pathologically were retrospectively analyzed. Inflammatory biomarkers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), and systemic immune-inflammation index (SII), were investigated.
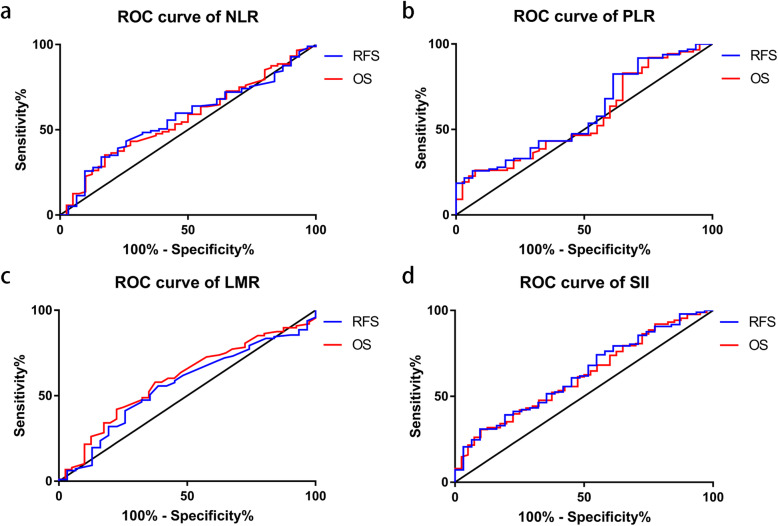
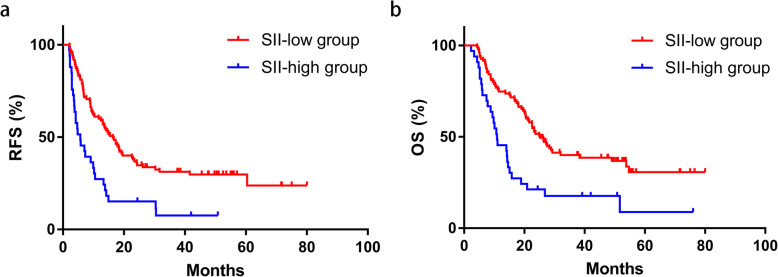
Receiver operating characteristic (ROC) curves showed no significance in NLR, PLR, and LMR in RFS and OS, while significant results were shown on SII in both RFS (P = 0.035) and OS (P = 0.034) with areas under ROC curve as 0.63 (95%CI 0.52-0.74) and 0.62 (95%CI 0.51-0.72), respectively. Kaplan-Meier curves revealed a statistically significant better survival data in SII-low groups on both RFS (P < 0.001) and OS (P < 0.001). The univariate and multivariate analyses revealed that higher level of SII was independently associated with both poorer RFS time and OS time. However, no significant result was shown on NLR, PLR, or LMR.
SII is an effective prognostic factor for predicting the prognosis of ICC patient undergone curative hepatectomy, while NLR, PLR, and LMR are not associated with clinical outcomes of these patients.
肝内胆管癌(ICC)是肝脏第二大常见恶性肿瘤,患者预后较差。越来越多的证据表明,炎症在肿瘤进展、血管生成和转移中起重要作用。然而,炎症生物标志物对 ICC 患者无复发生存(RFS)和总生存(OS)的预后意义尚未被认识。
回顾性分析接受根治性肝切除术并经病理诊断为 ICC 的患者。研究了炎症生物标志物,包括中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、淋巴细胞与单核细胞比值(LMR)和全身免疫炎症指数(SII)。
ROC 曲线显示 NLR、PLR 和 LMR 对 RFS 和 OS 无显著意义,而 SII 对 RFS(P = 0.035)和 OS(P = 0.034)均有显著意义,ROC 曲线下面积分别为 0.63(95%CI 0.52-0.74)和 0.62(95%CI 0.51-0.72)。Kaplan-Meier 曲线显示 SII 低值组在 RFS(P < 0.001)和 OS(P < 0.001)上均有显著的生存数据更好。单因素和多因素分析显示,较高的 SII 水平与 RFS 时间和 OS 时间较差均独立相关。然而,NLR、PLR 和 LMR 与临床结局无显著相关性。
SII 是预测接受根治性肝切除术的 ICC 患者预后的有效预后因素,而 NLR、PLR 和 LMR 与这些患者的临床结局无关。