Department of Liver Surgery and Liver Transplantation Center, West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China.
Laboratory of Liver Surgery, West China Hospital, Sichuan University, Chengdu 610065, Sichuan Province, China.
World J Gastroenterol. 2020 Apr 7;26(13):1501-1512. doi: 10.3748/wjg.v26.i13.1501.
Intrahepatic cholangiocarcinoma (ICC) is a heterogeneous hepatobiliary cancer with limited treatment options. A number of studies have illuminated the relationship between inflammation-based prognostic scores and outcomes in patients with ICC. However, the use of reliable and personalized prognostic algorithms in ICC after resection is pending.
To assess the prognostic value of the gamma-glutamyltransferase to lymphocyte ratio (GLR) in ICC patients following curative resection.
ICC patients following curative resection (2009-2017) were divided into two cohorts: The derivation cohort and validation cohort. The derivation cohort was used to explore an optimal cut-off value, and the validation cohort was used to further evaluate the score. Overall survival (OS) and recurrence-free survival (RFS) were analyzed, and predictors of OS and RFS were determined.
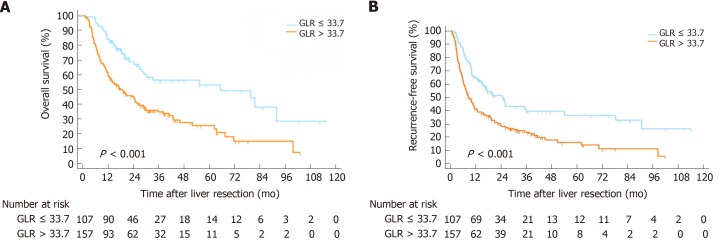
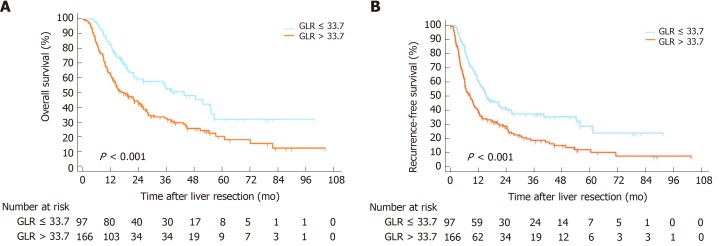
A total of 527 ICC patients were included and randomly divided into the derivation cohort (264 patients) and the validation cohort (263 patients). The two patient cohorts had comparable baseline characteristics. The optimal cut-off value for the GLR was 33.7. Kaplan-Meier curves showed worse OS and RFS in the GLR > 33.7 group compared with GLR ≤ 33.7 group in both cohorts. After univariate and multivariate analysis, the results indicated that GLR was an independent prognostic factor of OS [derivation cohort: hazard ratio (HR) = 1.620, 95% confidence interval (CI): 1.066-2.462, = 0.024; validation cohort: HR = 1.466, 95%CI: 1.033-2.142, = 0.048] and RFS [derivation cohort: HR = 1.471, 95%CI: 1.029-2.103, = 0.034; validation cohort: HR = 1.480, 95%CI: 1.057-2.070, = 0.022].
The preoperative GLR is an independent prognostic factor for ICC patients following hepatectomy. A high preoperative GLR is associated with worse OS and RFS.
肝内胆管细胞癌(ICC)是一种具有异质性的肝胆恶性肿瘤,治疗选择有限。许多研究阐明了炎症为基础的预后评分与 ICC 患者结局之间的关系。然而,在 ICC 切除术后,可靠和个性化的预后算法仍有待探索。
评估 γ-谷氨酰转肽酶与淋巴细胞比值(GLR)在 ICC 患者根治性切除术后的预后价值。
回顾性分析 2009 年至 2017 年接受根治性切除术的 ICC 患者,将患者分为两个队列:推导队列和验证队列。推导队列用于探索最佳截断值,验证队列用于进一步评估评分。分析总生存期(OS)和无复发生存期(RFS),确定 OS 和 RFS 的预测因素。
共纳入 527 例 ICC 患者,随机分为推导队列(264 例)和验证队列(263 例)。两组患者的基线特征具有可比性。GLR 的最佳截断值为 33.7。Kaplan-Meier 曲线显示,在两个队列中,GLR>33.7 组的 OS 和 RFS 均较 GLR≤33.7 组差。单因素和多因素分析结果表明,GLR 是 OS 的独立预后因素[推导队列:风险比(HR)=1.620,95%置信区间(CI):1.066-2.462,P=0.024;验证队列:HR=1.466,95%CI:1.033-2.142,P=0.048]和 RFS[推导队列:HR=1.471,95%CI:1.029-2.103,P=0.034;验证队列:HR=1.480,95%CI:1.057-2.070,P=0.022]。
术前 GLR 是 ICC 患者肝切除术后的独立预后因素。术前 GLR 升高与 OS 和 RFS 较差相关。