Jeong Rachel, Quinn Robert R, Ravani Pietro, Ye Feng, Sood Manish M, Massicotte-Azarniouch David, Tonelli Marcello, Hemmelgarn Brenda R, Lam Ngan N
Division of Nephrology, Cumming School of Medicine and the Department of Community Health Sciences, University of Calgary, AB, Canada.
Department of Medicine, Division of Nephrology, University of Alberta, Edmonton, Canada.
Can J Kidney Health Dis. 2020 Oct 8;7:2054358120952198. doi: 10.1177/2054358120952198. eCollection 2020.
Compared to the general population, kidney transplant recipients are at increased risk of hemorrhage and thrombosis. Whether this risk is affected by graft function and albuminuria is unknown.
To determine the association between graft function and albuminuria and the risk of post-transplant hemorrhage and thrombosis.
Retrospective cohort study.
We used linked health care databases in Alberta, Canada.
PATIENTS/SAMPLE/PARTICIPANTS: We included adult kidney transplant recipients from 2002 to 2015 with a functioning graft at 1 year.
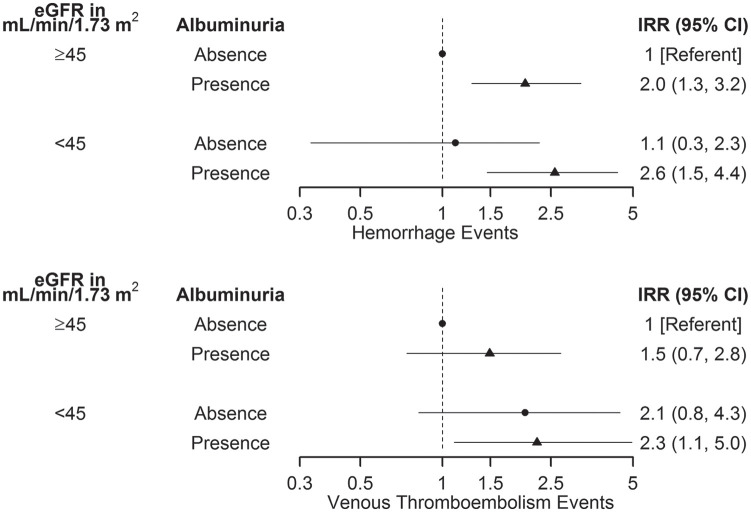
Estimated glomerular filtration rate (eGFR) and albuminuria measurements at 1 year post-transplant were used to categorize recipients (eGFR: ≥45 vs. <45 mL/min/1.73 m; albuminuria: absence vs. presence). We determined the rates of post-transplant hemorrhage and venous thrombosis based on validated diagnostic and procedural codes.
We determined the association between categories of eGFR and albuminuria and post-transplant hemorrhage and venous thrombosis using Poisson regression with log link.
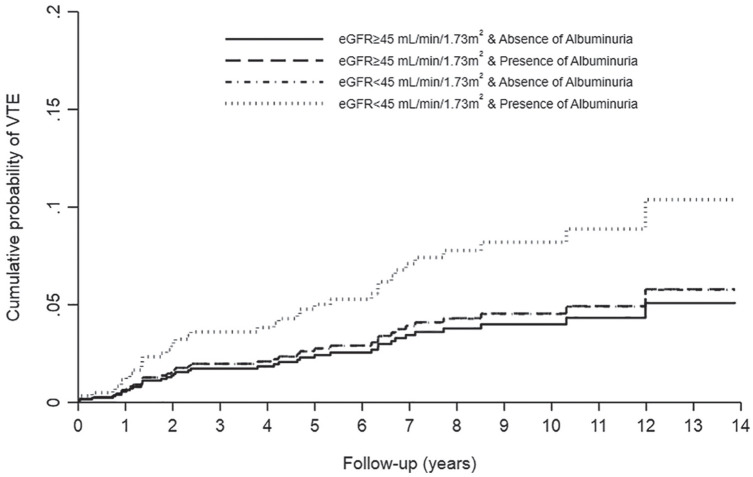
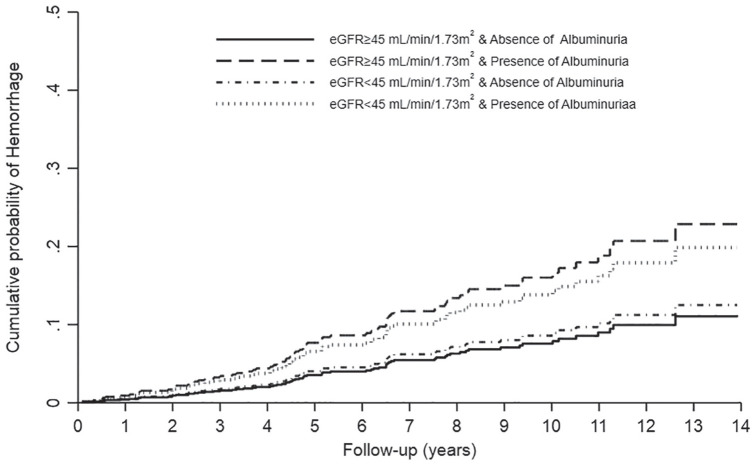
Of 1284 kidney transplant recipients, 21% had an eGFR <45 mL/min/1.73 m and 40% had presence of albuminuria at 1 year post-transplant. Over a median follow-up of 6 years, there were 100 hemorrhages (12.6 events per 1000 person-years) and 57 venous thrombosis events (7.1 events per 1000 person-years). The age- and sex-adjusted rate of hemorrhage and thrombosis was over 2-fold higher in recipients with lower eGFR and presence of albuminuria compared to higher eGFR and no albuminuria (hemorrhage: incidence rate ratio, IRR, 2.6, 95% confidence interval [CI]: 1.5-4.4, = .001; thrombosis: IRR, 2.3, 95% CI: 1.1-5.0, = .046).
Complete relevant medication information, such as anticoagulants, were not available in our datasets. Due to sample size, this study was underpowered to conduct a fully adjusted analysis.
Among kidney transplant recipients, lower eGFR and presence of albuminuria at 1 year post-transplant were associated with an over 2-fold higher risk of hemorrhage and venous thrombosis. Graft function and albuminuria at 1 year post-transplant are important prognostic factors in determining risk of post-transplant hemorrhage and venous thrombosis. Further research, including medication data, are needed to further delineate outcomes and safety.
Not applicable (cohort study).
与普通人群相比,肾移植受者出血和血栓形成的风险增加。这种风险是否受移植肾功能和蛋白尿的影响尚不清楚。
确定移植肾功能和蛋白尿与移植后出血和血栓形成风险之间的关联。
回顾性队列研究。
我们使用了加拿大艾伯塔省的关联医疗保健数据库。
患者/样本/参与者:我们纳入了2002年至2015年的成年肾移植受者,这些受者在1年时移植肾功能良好。
移植后1年的估计肾小球滤过率(eGFR)和蛋白尿测量值用于对受者进行分类(eGFR:≥45 vs. <45 mL/min/1.73 m²;蛋白尿:无 vs. 有)。我们根据经过验证的诊断和程序编码确定移植后出血和静脉血栓形成的发生率。
我们使用对数链接的泊松回归确定eGFR和蛋白尿类别与移植后出血和静脉血栓形成之间的关联。
在1284名肾移植受者中,21%的受者在移植后1年eGFR<45 mL/min/1.73 m²,40%的受者存在蛋白尿。在中位随访6年期间,有100例出血事件(每1000人年12.6例)和57例静脉血栓形成事件(每1000人年7.1例)。与eGFR较高且无蛋白尿的受者相比,eGFR较低且存在蛋白尿的受者经年龄和性别调整后的出血和血栓形成发生率高出2倍以上(出血:发病率比,IRR,2.6,95%置信区间[CI]:1.5 - 4.4,P = 0.001;血栓形成:IRR,2.3,95% CI:1.1 - 5.0,P = 0.046)。
我们的数据集中没有完整的相关药物信息,如抗凝剂。由于样本量的原因,本研究进行全面调整分析的能力不足。
在肾移植受者中,移植后1年eGFR较低和存在蛋白尿与出血和静脉血栓形成风险高出2倍以上相关。移植后1年的移植肾功能和蛋白尿是确定移植后出血和静脉血栓形成风险的重要预后因素。需要进一步的研究,包括药物数据,以进一步明确结果和安全性。
不适用(队列研究)。