Drakaki Alexandra, Dhillon Preet K, Wakelee Heather, Chui Stephen Y, Shim Jinjoo, Kent Matthew, Degaonkar Viraj, Hoang Tien, McNally Virginia, Luhn Patricia, Gutzmer Ralf
Division of Hematology/Oncology, David Geffen School of Medicine, University of California, Los Angeles, CA, USA.
Personalized Healthcare, Product Developmen, Genentech, Inc, South San Francisco, CA, USA.
Oncoimmunology. 2020 Oct 5;9(1):1824645. doi: 10.1080/2162402X.2020.1824645.
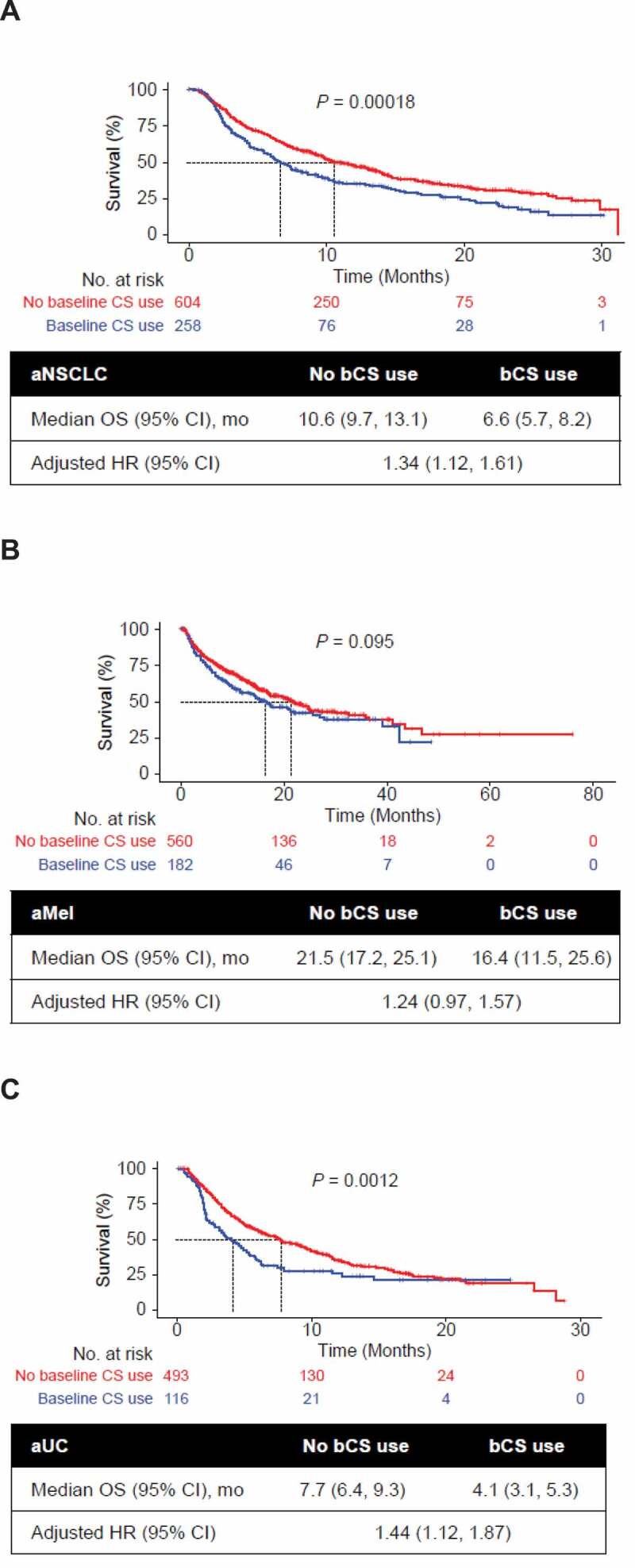
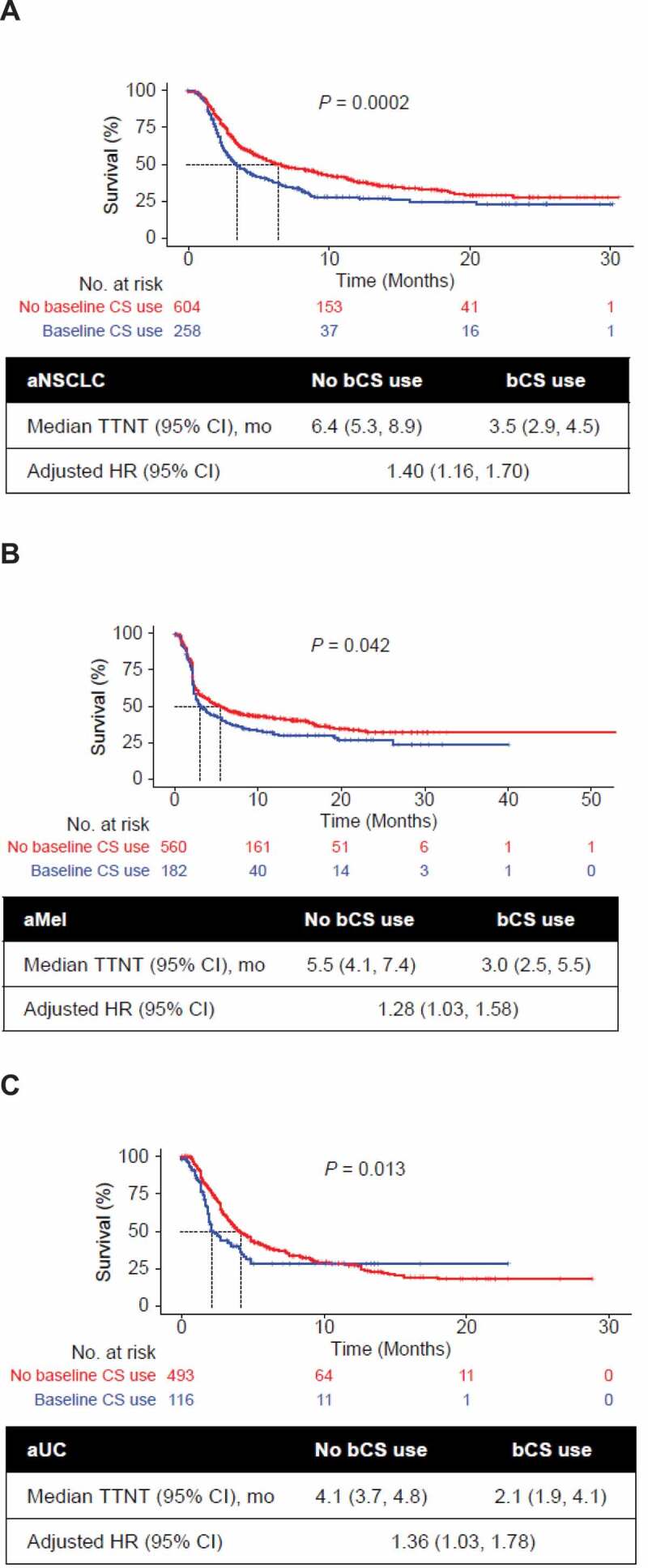
Immune checkpoint inhibitors (CPIs) have expanded treatment options for patients with solid tumors. Systemic corticosteroids (CSs) have an indispensable role in cancer care, but CS-related immunosuppression may counteract the CPI-driven antitumor immune response. This retrospective study investigated the association between baseline CS use (bCS; ≤14 days before, ≤30 days after CPI initiation) and clinical outcomes in patients with advanced non-small cell lung cancer (aNSCLC), melanoma (aMel), or urothelial carcinoma (aUC). We analyzed data from the Flatiron Health electronic health record-derived de-identified database for adults diagnosed with aNSCLC, aMel, or aUC between January 2011 and June 2017 who received ≥1 CPI monotherapy in any treatment line. Associations of bCS use with overall survival (OS) and time to next treatment (TTNT) were estimated using multivariable Cox proportional hazards models adjusting for demographic and clinical characteristics (i.e., ECOG performance status, site of metastases). In total, 2,213 patients were diagnosed with aNSCLC (n = 862), aMel (n = 742), or aUC (n = 609) and received ≥1 CPI administration. Most patients (67%-95%) received CSs, many during the baseline period (19%-30%). Patients with bCS use had shorter median OS than those with no bCS use for aNSCLC (6.6 vs 10.6 months; = .00018), aMel (16.4 vs 21.5; = .095), and aUC (4.1 vs 7.7; = .0012). bCS use was associated with shorter OS (not significant for aMel) and TTNT in adjusted multivariable analyses, and clinical outcomes were not explained by prior CS use or other measured confounders. These findings suggest a potential association between bCS use and decreased CPI effectiveness, warranting further investigation.
免疫检查点抑制剂(CPI)为实体瘤患者拓展了治疗选择。全身用糖皮质激素(CS)在癌症治疗中发挥着不可或缺的作用,但与CS相关的免疫抑制可能会抵消CPI驱动的抗肿瘤免疫反应。这项回顾性研究调查了晚期非小细胞肺癌(aNSCLC)、黑色素瘤(aMel)或尿路上皮癌(aUC)患者基线期使用CS(bCS;CPI开始前≤14天、开始后≤30天)与临床结局之间的关联。我们分析了来自Flatiron Health电子健康记录去识别数据库的数据,该数据库涵盖了2011年1月至2017年6月期间被诊断为aNSCLC、aMel或aUC且在任何治疗线接受≥1次CPI单药治疗的成年人。使用多变量Cox比例风险模型估计bCS使用与总生存期(OS)和下次治疗时间(TTNT)之间的关联,并对人口统计学和临床特征(即东部肿瘤协作组体能状态、转移部位)进行校正。共有2213例患者被诊断为aNSCLC(n = 862)、aMel(n = 742)或aUC(n = 609)并接受了≥1次CPI给药。大多数患者(67%-95%)接受了CS,许多是在基线期(19%-30%)。对于aNSCLC,使用bCS的患者中位OS短于未使用bCS的患者(6.6个月对10.6个月;P = 0.00018),aMel患者(16.4个月对21.5个月;P = 0.095),aUC患者(4.1个月对7.7个月;P = 0.0012)。在多变量校正分析中,使用bCS与较短的OS(aMel不显著)和TTNT相关,且临床结局无法通过既往使用CS或其他测量的混杂因素来解释。这些发现提示bCS使用与CPI有效性降低之间可能存在关联,值得进一步研究。