SingHealth Duke-NUS Emergency Medicine Academic Clinical Programme Singapore.
Pre-Hospital & Emergency Research Centre Duke-NUS Medical School Singapore.
J Am Heart Assoc. 2020 Nov 3;9(21):e015368. doi: 10.1161/JAHA.119.015368. Epub 2020 Oct 26.
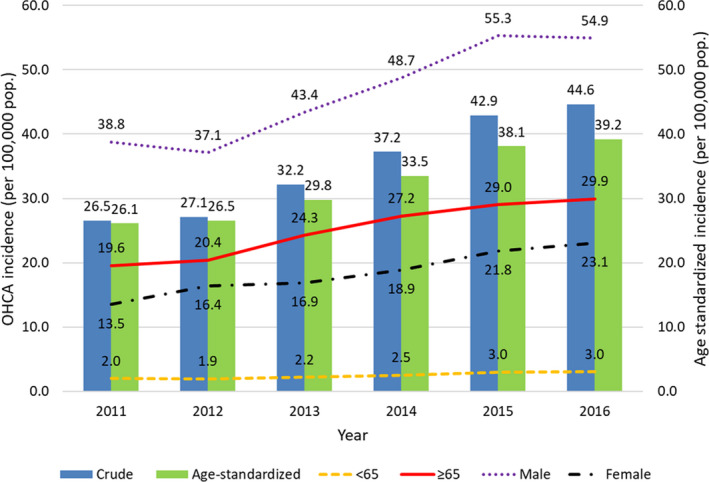
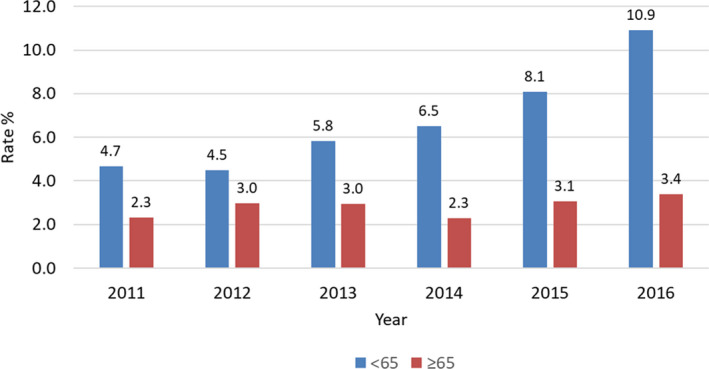
Background Outcomes of patients from out-of-hospital cardiac arrest (OHCA) vary widely globally because of differences in prehospital systems of emergency care. National efforts had gone into improving OHCA outcomes in Singapore in recent years including community and prehospital initiatives. We aimed to document the impact of implementation of a national 5-year Plan for prehospital emergency care in Singapore on OHCA outcomes from 2011 to 2016. Methods and Results Prospective, population-based data of OHCA brought to Emergency Departments were obtained from the Pan-Asian Resuscitation Outcomes Study cohort. The primary outcome was Utstein (bystander witnessed, shockable rhythm) survival-to-discharge or 30-day postarrest. Mid-year population estimates were used to calculate age-standardized incidence. Multivariable logistic regression was performed to identify prehospital characteristics associated with survival-to-discharge across time. A total of 11 465 cases qualified for analysis. Age-standardized incidence increased from 26.1 per 100 000 in 2011 to 39.2 per 100 000 in 2016. From 2011 to 2016, Utstein survival rates nearly doubled from 11.6% to 23.1% (=0.006). Overall survival rates improved from 3.6% to 6.5% (<0.001). Bystander cardiopulmonary resuscitation rates more than doubled from 21.9% to 56.3% and bystander automated external defibrillation rates also increased from 1.8% to 4.6%. Age ≤65 years, nonresidential location, witnessed arrest, shockable rhythm, bystander automated external defibrillation, and year 2016 were independently associated with improved survival. Conclusions Implementation of a national prehospital strategy doubled OHCA survival in Singapore from 2011 to 2016, along with corresponding increases in bystander cardiopulmonary resuscitation and bystander automated external defibrillation. This can be an implementation model for other systems trying to improve OHCA outcomes.
由于院外心脏骤停 (OHCA) 患者在院外急救系统方面存在差异,全球各国的患者预后存在很大差异。近年来,新加坡一直在努力改善 OHCA 患者的预后,包括社区和院外急救方面的措施。本研究旨在记录 2011 年至 2016 年期间,新加坡实施国家 5 年院前急救计划对 OHCA 预后的影响。
前瞻性、基于人群的 OHCA 患者数据来自泛亚复苏结果研究队列。主要结局为乌斯丁(目击者、可除颤节律)存活至出院或复苏后 30 天。采用年中人口估计数计算年龄标准化发病率。采用多变量逻辑回归确定随时间变化与存活至出院相关的院前特征。共有 11465 例符合分析条件。年龄标准化发病率从 2011 年的 26.1/100000 上升到 2016 年的 39.2/100000。从 2011 年到 2016 年,乌斯丁生存率从 11.6%上升到 23.1%(=0.006)。总体生存率从 3.6%上升到 6.5%(<0.001)。旁观者心肺复苏率从 21.9%上升到 56.3%,旁观者自动体外除颤率从 1.8%上升到 4.6%。年龄≤65 岁、非居住地点、目击性骤停、可除颤节律、旁观者自动体外除颤和 2016 年是与生存率提高相关的独立因素。
2011 年至 2016 年,新加坡实施国家院前急救策略使 OHCA 生存率提高了一倍,同时旁观者心肺复苏和旁观者自动体外除颤的比例也相应增加。这可为其他试图改善 OHCA 预后的系统提供实施模式。