Little Callum D, Kotecha Tushar, Candilio Luciano, Jabbour Richard J, Collins George B, Ahmed Asrar, Connolly Michelle, Kanyal Ritesh, Demir Ozan M, Lawson Lucy O, Wang Brian, Firoozi Sam, Spratt James C, Perera Divaka, MacCarthy Philip, Dalby Miles, Jain Ajay, Wilson Simon J, Malik Iqbal, Rakhit Roby
Department of Cardiology, Royal Free London NHS Foundation Trust, London, United Kingdom
Institute of Cardiovascular Science, University College London, London, United Kingdom.
Open Heart. 2020 Oct;7(2). doi: 10.1136/openhrt-2020-001432.
To understand the impact of COVID-19 on delivery and outcomes of primary percutaneous coronary intervention (PPCI). Furthermore, to compare clinical presentation and outcomes of patients with ST-segment elevation myocardial infarction (STEMI) with active COVID-19 against those without COVID-19.
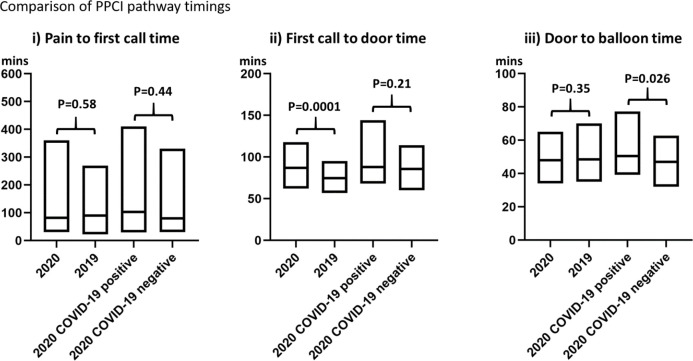
We systematically analysed 348 STEMI cases presenting to the PPCI programme in London during the peak of the pandemic (1 March to 30 April 2020) and compared with 440 cases from the same period in 2019. Outcomes of interest included ambulance response times, timeliness of revascularisation, angiographic and procedural characteristics, and in-hospital clinical outcomes RESULTS: There was a 21% reduction in STEMI admissions and longer ambulance response times (87 (62-118) min in 2020 vs 75 (57-95) min in 2019, p<0.001), but that this was not associated with a delays in achieving revascularisation once in hospital (48 (34-65) min in 2020 vs 48 (35-70) min in 2019, p=0.35) or increased mortality (10.9% (38) in 2020 vs 8.6% (38) in 2019, p=0.28). 46 patients with active COVID-19 were more thrombotic and more likely to have intensive care unit admissions (32.6% (15) vs 9.3% (28), OR 5.74 (95%CI 2.24 to 9.89), p<0.001). They also had increased length of stay (4 (3-9) days vs 3 (2-4) days, p<0.001) and a higher mortality (21.7% (10) vs 9.3% (28), OR 2.72 (95% CI 1.25 to 5.82), p=0.012) compared with patients having PPCI without COVID-19.
These findings suggest that PPCI pathways can be maintained during unprecedented healthcare emergencies but confirms the high mortality of STEMI in the context of concomitant COVID-19 infection characterised by a heightened state of thrombogenicity.
了解新型冠状病毒肺炎(COVID-19)对直接经皮冠状动脉介入治疗(PPCI)的实施及结果的影响。此外,比较合并活动性COVID-19的ST段抬高型心肌梗死(STEMI)患者与未感染COVID-19的患者的临床表现及结果。
我们系统分析了在疫情高峰期(2020年3月1日至4月30日)伦敦PPCI项目中收治的348例STEMI病例,并与2019年同期的440例病例进行比较。感兴趣的结果包括救护车响应时间、血运重建的及时性、血管造影和手术特征以及住院临床结果。结果:STEMI入院人数减少了21%,救护车响应时间延长(2020年为87(62 - 118)分钟,2019年为75(57 - 95)分钟,p<0.001),但这与住院后实现血运重建的延迟无关(2020年为48(34 - 65)分钟,2019年为48(35 - 70)分钟,p = 0.35),也与死亡率增加无关(2020年为10.9%(38例),2019年为8.6%(38例),p = 0.28)。46例合并活动性COVID-19的患者血栓形成更多,更有可能入住重症监护病房(32.6%(15例)对9.3%(28例),比值比5.74(95%置信区间2.24至9.89),p<0.001)。与未感染COVID-19而接受PPCI的患者相比,他们的住院时间也更长(4(3 - 9)天对3(2 - 4)天,p<0.001),死亡率更高(21.7%(10例)对9.3%(28例),比值比2.72(95%置信区间1.25至5.82),p = 0.012)。
这些发现表明,在前所未有的医疗紧急情况下,PPCI途径可以维持,但证实了在合并COVID-19感染的情况下STEMI的高死亡率,其特征是血栓形成倾向增强。