Nicol Martin, Cacoub Lea, Baudet Mathilde, Nahmani Yoram, Cacoub Patrice, Cohen-Solal Alain, Henry Patrick, Adle-Biassette Homa, Logeart Damien
Cardiology Department, APHP, Lariboisiere Hospital, Paris, France.
Internal Medicine Department, APHP, Pitie-Salpetriere Hospital, Paris, France.
ESC Heart Fail. 2020 Dec;7(6):4371-4376. doi: 10.1002/ehf2.13047. Epub 2020 Oct 26.
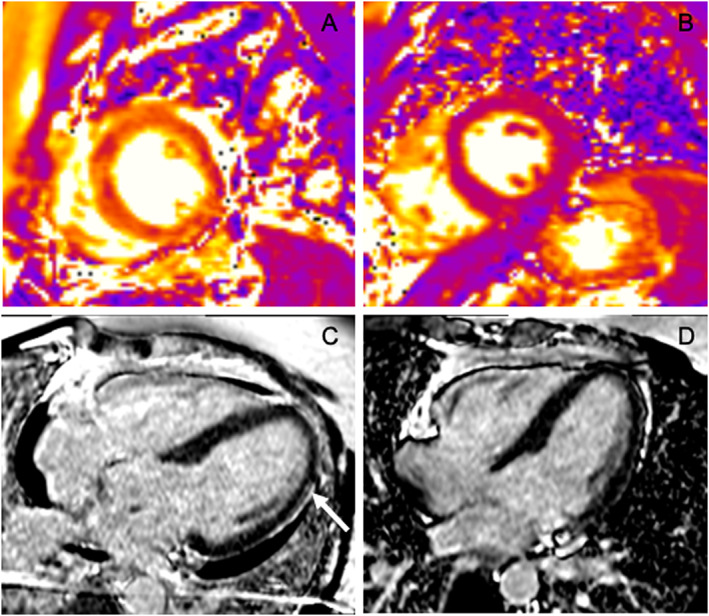
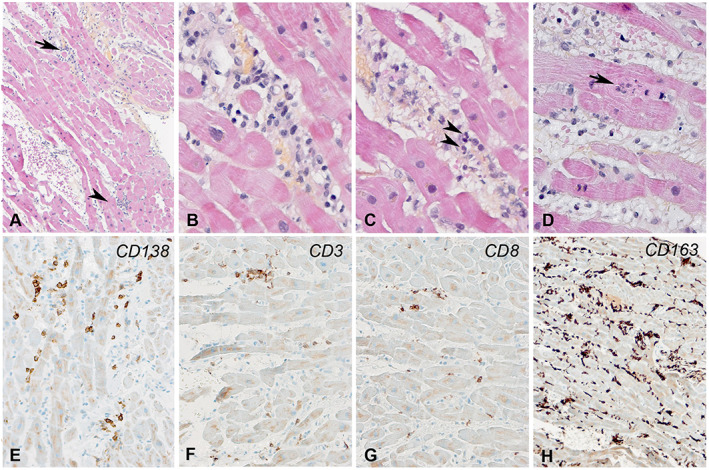
Precise descriptions of coronavirus disease 2019 (COVID-19)-related cardiac damage as well as underlying mechanisms are scarce. We describe clinical presentation and diagnostic workup of acute myocarditis in a patient who had developed COVID-19 syndrome 1 month earlier. A healthy 40-year-old man suffered from typical COVID-19 symptoms. Four weeks later, he was admitted because of fever and tonsillitis. Blood tests showed major inflammation. Thoracic computed tomography was normal, and RT-PCR for SARS-CoV-2 on nasopharyngeal swab was negative. Because of haemodynamic worsening with both an increase in cardiac troponin and B-type natriuretic peptide levels and normal electrocardiogram, acute myocarditis was suspected. Cardiac echographic examination showed left ventricular ejection fraction at 45%. Exhaustive diagnostic workup included RT-PCR and serologies for infectious agents and autoimmune blood tests as well as cardiac magnetic resonance imaging and endomyocardial biopsies. Cardiac magnetic resonance with T2 mapping sequences showed evidence of myocardial inflammation and focal lateral subepicardial late gadolinium enhancement. Pathological analysis exhibited interstitial oedema, small foci of necrosis, and infiltrates composed of plasmocytes, T-lymphocytes, and mainly CD163 macrophages. These findings led to the diagnosis of acute lympho-plasmo-histiocytic myocarditis. There was no evidence of viral RNA within myocardium. The only positive viral serology was for SARS-CoV-2. The patient and his cardiac function recovered in the next few days without use of anti-inflammatory or antiviral drugs. This case highlights that systemic inflammation associated with acute myocarditis can be delayed up to 1 month after initial SARS-CoV-2 infection and can be resolved spontaneously.
关于2019冠状病毒病(COVID-19)相关心脏损伤及其潜在机制的精确描述较为匮乏。我们描述了一名1个月前患上COVID-19综合征的患者急性心肌炎的临床表现及诊断检查过程。一名40岁健康男性出现了典型的COVID-19症状。四周后,他因发热和扁桃体炎入院。血液检查显示有严重炎症。胸部计算机断层扫描正常,鼻咽拭子的SARS-CoV-2逆转录聚合酶链反应(RT-PCR)检测为阴性。由于心脏肌钙蛋白和B型利钠肽水平升高且心电图正常,但血流动力学恶化,怀疑为急性心肌炎。心脏超声检查显示左心室射血分数为45%。详尽的诊断检查包括针对感染因子的RT-PCR和血清学检查、自身免疫性血液检查以及心脏磁共振成像和心内膜心肌活检。采用T2映射序列的心脏磁共振成像显示有心肌炎症及局灶性外侧心外膜下晚期钆增强的证据。病理分析显示有间质水肿、小灶性坏死以及由浆细胞、T淋巴细胞和主要为CD163巨噬细胞组成的浸润。这些发现确诊为急性淋巴细胞 - 浆细胞 - 组织细胞性心肌炎。心肌内未发现病毒RNA证据。唯一呈阳性的病毒血清学检查是针对SARS-CoV-2的。在接下来的几天里,患者及其心脏功能在未使用抗炎或抗病毒药物的情况下恢复。该病例突出表明,与急性心肌炎相关的全身炎症可能在初次感染SARS-CoV-2后延迟长达1个月出现,且可自发缓解。