Ye Senlin, Wang Haohui, He Kancheng, Peng Mou, Wang Yinhuai, Li Yuanwei, Jiang Shusuan, Li Jin, Yi Lu, Cui Rongrong
Department of Urology, The Second Xiangya Hospital of Central South University, Changsha, China.
Department of Urology, Hunan Provincial People's Hospital, Changsha, China.
Front Oncol. 2020 Oct 7;10:533282. doi: 10.3389/fonc.2020.533282. eCollection 2020.
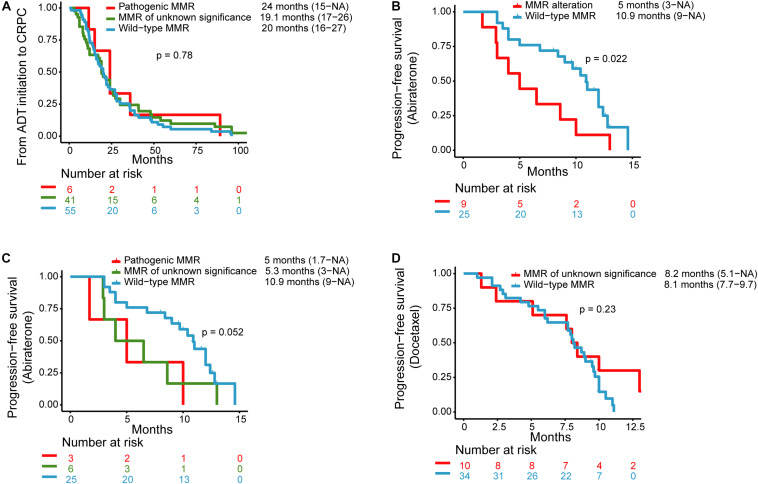
Mismatch repair-deficient (dMMR) prostate cancer is rare and has not been well studied. We aimed to evaluate the clinical characterization of dMMR metastatic castration-resistant prostate cancer (mCRPC) patients. The MMR genes include MLH1, MLH3, MSH2, MSH6, PMS1, PMS2, and EPCAM, and were analyzed by targeted sequencing of plasma cell-free DNA samples. A total of 109 mCRPC patients were identified, including 50 patients with MMR alterations (pathogenic alterations, = 7; alterations of unknown significance, = 43) and 59 patients with wild-type MMR. For the seven patients with pathogenic MMR alterations, the median age at diagnosis was 63.5 years, and 42.9% had a Gleason score ≥8. The median time from androgen deprivation therapy (ADT) initiation to CRPC was 24 months. Compared with the wild-type MMR subgroup, patients with MMR alterations, pathogenic MMR alterations, or MMR alterations of unknown significance showed higher rates of hotspot missense mutations or copy number amplifications in the AR gene (24/50 vs. 10/59, = 7.8 × 10; 7/7 vs. 10/59, = 2.5 × 10; 17/43 vs. 10/59, = 0.013). The presence of any MMR alterations was associated with an inferior response to abiraterone [median progression-free survival (PFS): 5.0 vs. 10.9 months, = 0.022]. Shorter PFS times were observed in both the pathogenic MMR alteration subgroup (median PFS: 5 months) and the MMR alterations of unknown significance subgroup (median PFS: 5.3 months), compared with the PFS of those with wild-type MMR genes (median PFS: 10.9 months, = 0.052). There was no statistically significant difference in response to docetaxel chemotherapy between the MMR alterations of unknown significance and the wild-type MMR subgroups (median PFS: 8.2 vs. 8.1 months, = 0.23). Our results demonstrate that dMMR mCRPC patients have an equivalent response to standard ADT and taxane-based chemotherapy treatments compared with wild-type MMR patients. Patients with both pathogenic and unknown significance alterations of MMR genes had poorer responses to abiraterone therapy.
错配修复缺陷(dMMR)前列腺癌较为罕见,尚未得到充分研究。我们旨在评估dMMR转移性去势抵抗性前列腺癌(mCRPC)患者的临床特征。错配修复(MMR)基因包括MLH1、MLH3、MSH2、MSH6、PMS1、PMS2和EPCAM,并通过对血浆游离DNA样本进行靶向测序来分析。共鉴定出109例mCRPC患者,其中50例存在MMR改变(致病性改变,n = 7;意义未明的改变,n = 43),59例为MMR野生型。对于7例致病性MMR改变的患者,诊断时的中位年龄为63.5岁,42.9%的患者Gleason评分≥8。从雄激素剥夺治疗(ADT)开始至CRPC的中位时间为24个月。与MMR野生型亚组相比,存在MMR改变、致病性MMR改变或意义未明的MMR改变的患者,AR基因中的热点错义突变或拷贝数扩增发生率更高(24/50 vs. 10/59,P = 7.8×10⁻²;7/7 vs. 10/59,P = 2.5×10⁻³;17/43 vs. 10/59,P = 0.013)。任何MMR改变的存在与阿比特龙治疗反应较差相关[中位无进展生存期(PFS):5.0个月 vs. 10.9个月,P = 0.022]。与MMR基因野生型患者的PFS(中位PFS:10.9个月)相比,致病性MMR改变亚组(中位PFS:5个月)和意义未明的MMR改变亚组(中位PFS:5.3个月)的PFS时间均较短(P = 0.052)。意义未明的MMR改变亚组与MMR野生型亚组在多西他赛化疗反应方面无统计学显著差异(中位PFS:8.2个月 vs. 8.1个月,P = 0.23)。我们的结果表明,与MMR野生型患者相比,dMMR mCRPC患者对标准ADT和基于紫杉烷的化疗治疗反应相当。MMR基因存在致病性和意义未明改变的患者对阿比特龙治疗反应较差。