Jensen Bente Thoft, Lauridsen Susanne Vahr, Jensen Jørgen Bjerggaard
Department of Urology, Aarhus University Hospital, Aarhus, Denmark.
Department of Urology, Copenhagen University Hospital, Denmark and WHO-CC, Clinical Health Promotion Centre, The Parker Institute Bispebjerg & Frederiksberg University Hospital, Copenhagen, Denmark.
Res Rep Urol. 2020 Oct 14;12:471-486. doi: 10.2147/RRU.S270240. eCollection 2020.
To identify components representing optimal delivery of follow-up care after radical cystectomy because of bladder cancer and report the current level of evidence.
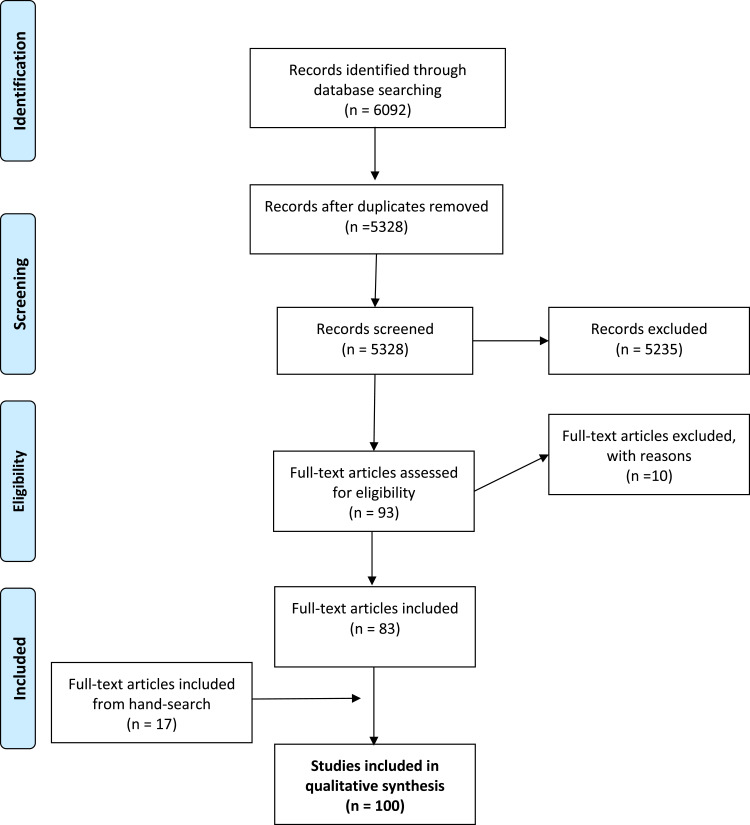
We conducted a systematic literature search of the following databases: Cochrane, MEDLINE, Embase, CINAHL, Web of Science, Physiotherapy Evidence Database and ClinicalTrials.gov. The search results were managed in Covidence Reference Manager and abstracts were screened by title. Articles relevant to the subject of interest were included and the results are reported narratively.
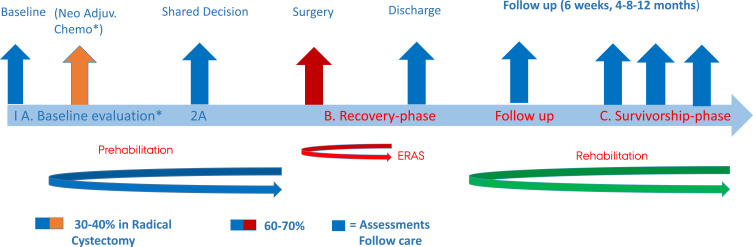
Several studies have evaluated the positive impact of enhanced recovery after surgery (ERAS) on length of stay, albeit not on the further impact on 90-day postoperative complication rate, functional recovery, or mortality. Minimally invasive surgery may result in a slighter shorter length of stay compared to open surgery. Physical training combined with nutritional intervention can improve functional recovery up to one year after surgery. Nutritional supplements can preserve muscle and bone mass, and potentially improve recovery. Patient education in stoma care and prevention of infection can significantly improve self-efficacy and avoid symptoms of infection postoperatively. Moreover, specific devices like applications (apps) can support these efforts. Continued smoking increases the risk of developing postoperative complications while no evidence was found on the impact of continued alcohol drinking. Currently, there is no evidence on psychological well-being, sexual health, or shared decision making interventions with an impact on rehabilitation after radical cystectomy.
Data are scarce but indicate that peri- and postoperative multi-professional interventions can reduce prevalence of sarcopenia, and improve functional recovery, physical capacity, nutritional status, and self-efficacy in stoma care (level 1 evidence). Continued smoking increases the risk of complications, but the effects of a smoking and alcohol intervention remain unclear (level 3 evidence). The results of this review provide guidance for future directions in research and further attempts to develop and test an evidence-based program for follow-up care after radical cystectomy.
确定膀胱癌根治性膀胱切除术后随访护理最佳实施的组成部分,并报告当前的证据水平。
我们对以下数据库进行了系统的文献检索:Cochrane、MEDLINE、Embase、CINAHL、Web of Science、物理治疗证据数据库和ClinicalTrials.gov。检索结果在Covidence参考文献管理器中进行管理,并通过标题筛选摘要。纳入了与感兴趣主题相关的文章,并以叙述方式报告结果。
多项研究评估了术后加速康复(ERAS)对住院时间的积极影响,尽管未评估其对术后90天并发症发生率、功能恢复或死亡率的进一步影响。与开放手术相比,微创手术可能会使住院时间略短。体育锻炼与营养干预相结合可改善术后长达一年的功能恢复。营养补充剂可维持肌肉和骨量,并可能改善恢复情况。造口护理和感染预防方面的患者教育可显著提高自我效能,并避免术后感染症状。此外,应用程序等特定设备可支持这些工作。持续吸烟会增加术后并发症的发生风险,而未发现持续饮酒的影响。目前,尚无证据表明心理幸福感、性健康或共同决策干预对根治性膀胱切除术后的康复有影响。
数据稀缺,但表明围手术期和术后的多专业干预可降低肌肉减少症的患病率,并改善功能恢复、身体能力、营养状况和造口护理方面的自我效能(1级证据)。持续吸烟会增加并发症风险,但吸烟和饮酒干预的效果仍不明确(3级证据)。本综述结果为未来研究方向提供了指导,并为进一步尝试制定和测试根治性膀胱切除术后随访护理的循证方案提供了依据。