Liu Miaoxia, Wu Ruihong, Liu Xu, Xu Hongqin, Chi Xiumei, Wang Xiaomei, Zhan Mengru, Wang Bao, Peng Fei, Gao Xiuzhu, Shi Ying, Wen Xiaoyu, Ji Yali, Jin Qinglong, Niu Junqi
Department of Hepatology, First Hospital of Jilin University, Changchun, Jilin Province 130021, People's Republic of China.
Hepatology Unit, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou 510515, People's Republic of China.
J Hepatocell Carcinoma. 2020 Oct 23;7:219-232. doi: 10.2147/JHC.S271790. eCollection 2020.
GALAD is a statistical model for estimating the likelihood of having hepatocellular carcinoma (HCC) based on gender, age, AFP, AFP-L3, and PIVKA-II. We aimed to assess its performance and build new models in China, where hepatitis B virus (HBV) is the leading etiology of HCC.
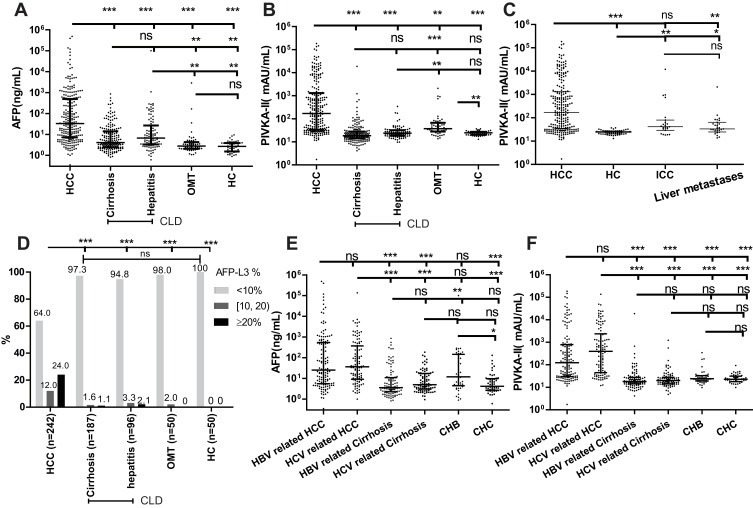
We built the GALAD-C model with the same five variables in GALAD, and the GAAP model with gender, age, AFP, and PIVKA-II, using logistic regression based on 242 patients with HCC and 283 patients with chronic liver disease (CLD). We also collected 50 patients with other malignant liver tumors (OMTs) and 50 healthy controls (HCs). A test dataset (169 patients with HCC and 139 with CLD) was used to test the performance of GAAP.
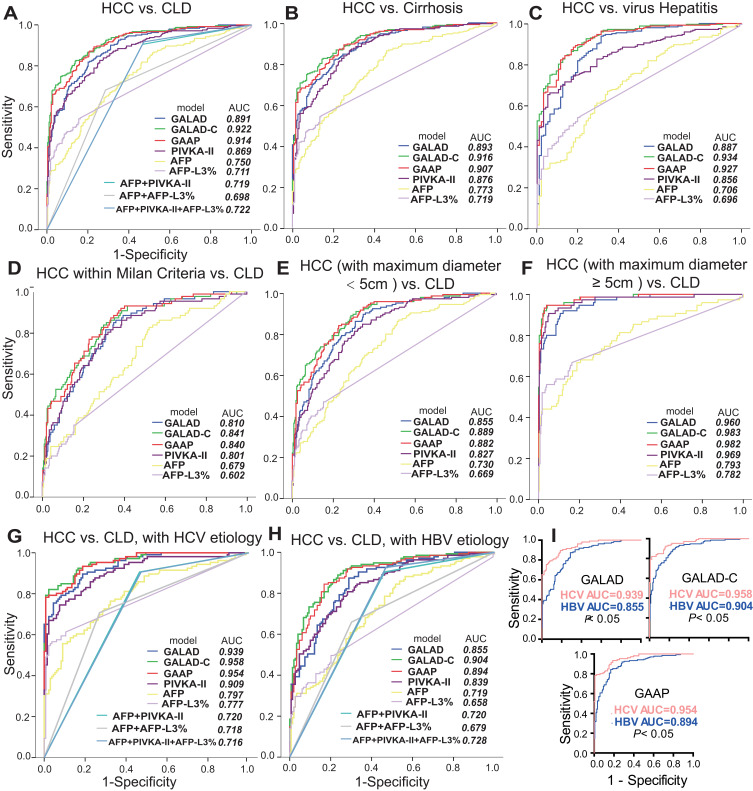
The GALAD-C and GAAP models achieved comparable performance (area under the receiver operating characteristic curve [AUC], 0.922 vs 0.914), and both were superior to GALAD, PIVKA-II, AFP, and AFP-L3% (AUCs, 0.891, 0.869, 0.750, and 0.711) for discrimination of HCC from CLD for the entire dataset. The AUCs of the GALAD, GALAD-C and GAAP models were excellent for the hepatitis C virus (HCV) subgroup (0.939, 0.958 and 0.954), and for discrimination HCC from HCs (0.988, 0.982, and 0.979), but were relatively lower for the HBV subgroup (0.855, 0.904, and 0.894), and for HCC within Milan Criteria (0.810, 0.841, and 0.840). They were not superior to AFP (0.873) for discrimination of HCC from OMT (0.873, 0.809, and 0.823). GAAP achieved an AUC of 0.922 in the test dataset.
GALAD was excellent for discrimination of HCC from CLD in the HCV subgroup of a cohort of Chinese patients. The GAAP and GALAD-C models achieved better performance compared with GALAD. These three models exhibited better performance in patients with an HCV etiology than those with HBV.
GALAD是一种基于性别、年龄、甲胎蛋白(AFP)、甲胎蛋白-L3(AFP-L3)和异常凝血酶原(PIVKA-II)来估计肝细胞癌(HCC)发生可能性的统计模型。我们旨在评估其性能,并在中国建立新模型,在中国,乙型肝炎病毒(HBV)是HCC的主要病因。
我们使用基于242例HCC患者和283例慢性肝病(CLD)患者的逻辑回归,构建了与GALAD具有相同五个变量的GALAD-C模型,以及包含性别、年龄、AFP和PIVKA-II的GAAP模型。我们还收集了50例其他肝脏恶性肿瘤(OMT)患者和50例健康对照(HC)。一个测试数据集(169例HCC患者和139例CLD患者)用于测试GAAP的性能。
GALAD-C模型和GAAP模型具有相当的性能(受试者操作特征曲线下面积[AUC],分别为0.922和0.914),并且在区分整个数据集中的HCC和CLD方面,两者均优于GALAD、PIVKA-II、AFP和AFP-L3%(AUC分别为0.891、0.869、0.750和0.711)。GALAD、GALAD-C和GAAP模型在丙型肝炎病毒(HCV)亚组中区分HCC和CLD的AUC(分别为0.939、0.958和0.954)以及区分HCC和HC的AUC(分别为0.988、0.982和0.979)方面表现出色,但在HBV亚组中(分别为0.855、0.904和0.894)以及在米兰标准内的HCC中(分别为0.810、0.841和0.840)相对较低。在区分HCC和OMT方面(分别为0.873、0.809和0.823),它们并不优于AFP(0.873)。GAAP在测试数据集中的AUC为0.922。
在一组中国患者的HCV亚组中,GALAD在区分HCC和CLD方面表现出色。与GALAD相比,GAAP和GALAD-C模型表现更好。这三种模型在病因是HCV的患者中比病因是HBV的患者表现更好。