Department of Melanoma Medical Oncology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX, 77030, USA.
Immunitas Therapeutics, Cambridge, MA, USA.
Cancer Immunol Immunother. 2021 Apr;70(4):1101-1113. doi: 10.1007/s00262-020-02748-9. Epub 2020 Oct 29.
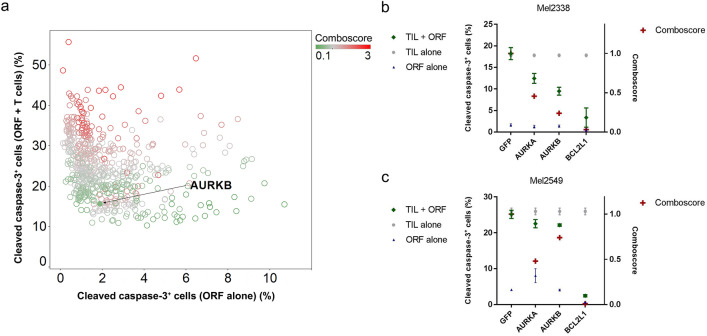
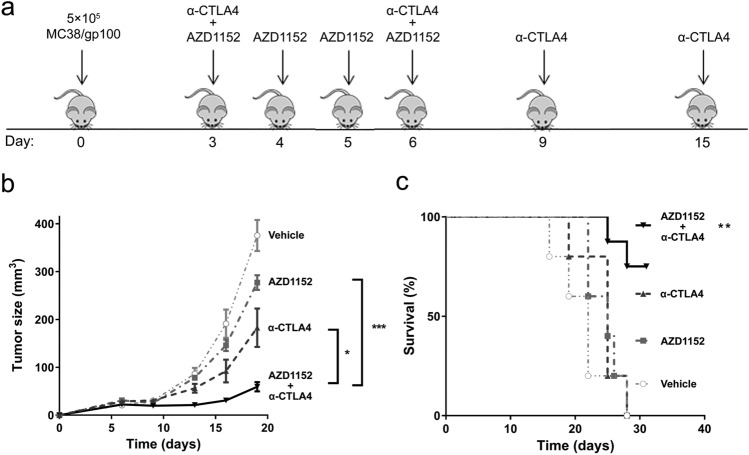
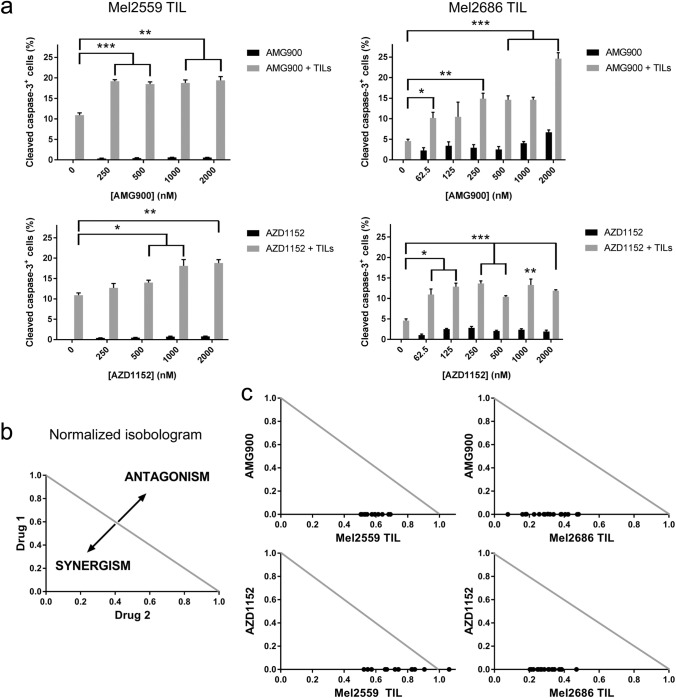
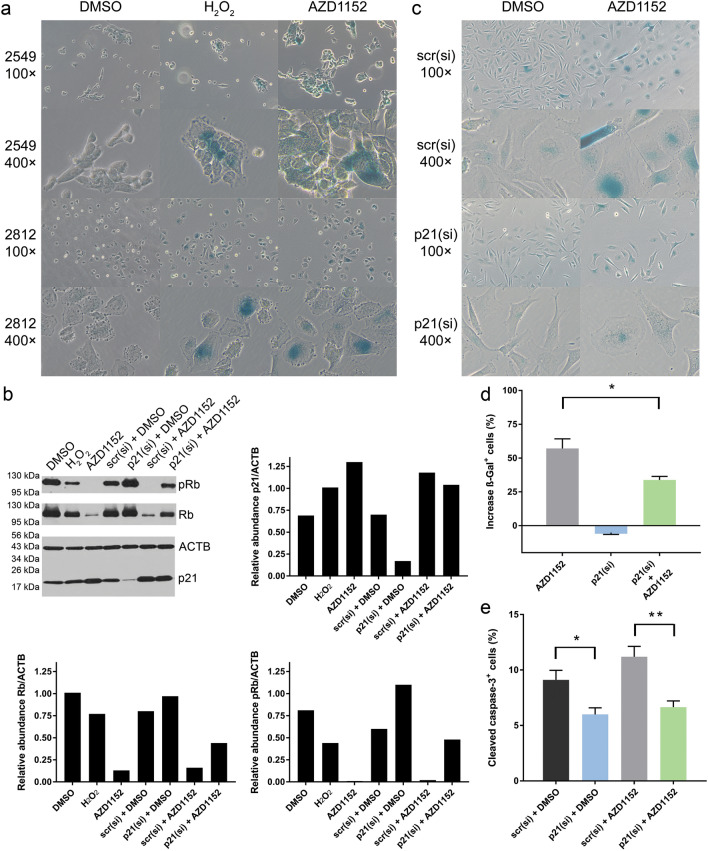
Although immunotherapy has achieved impressive durable clinical responses, many cancers respond only temporarily or not at all to immunotherapy. To find novel, targetable mechanisms of resistance to immunotherapy, patient-derived melanoma cell lines were transduced with 576 open reading frames, or exposed to arrayed libraries of 850 bioactive compounds, prior to co-culture with autologous tumor-infiltrating lymphocytes (TILs). The synergy between the targets and TILs to induce apoptosis, and the mechanisms of inhibiting resistance to TILs were interrogated. Gene expression analyses were performed on tumor samples from patients undergoing immunotherapy for metastatic melanoma. Finally, the effect of inhibiting the top targets on the efficacy of immunotherapy was investigated in multiple preclinical models. Aurora kinase was identified as a mediator of melanoma cell resistance to T-cell-mediated cytotoxicity in both complementary screens. Aurora kinase inhibitors were validated to synergize with T-cell-mediated cytotoxicity in vitro. The Aurora kinase inhibition-mediated sensitivity to T-cell cytotoxicity was shown to be partially driven by p21-mediated induction of cellular senescence. The expression levels of Aurora kinase and related proteins were inversely correlated with immune infiltration, response to immunotherapy and survival in melanoma patients. Aurora kinase inhibition showed variable responses in combination with immunotherapy in vivo, suggesting its activity is modified by other factors in the tumor microenvironment. These data suggest that Aurora kinase inhibition enhances T-cell cytotoxicity in vitro and can potentiate antitumor immunity in vivo in some but not all settings. Further studies are required to determine the mechanism of primary resistance to this therapeutic intervention.
虽然免疫疗法已经取得了令人瞩目的持久临床疗效,但许多癌症对免疫疗法的反应只是暂时的,或者根本没有反应。为了寻找新的、可靶向的免疫疗法耐药机制,将 576 个开放阅读框转导到患者来源的黑色素瘤细胞系中,或者将其暴露于 850 种生物活性化合物的阵列文库中,然后与自体肿瘤浸润淋巴细胞(TIL)共培养。在诱导细胞凋亡方面,研究了靶点与 TIL 之间的协同作用,以及抑制 TIL 耐药的机制。对接受转移性黑色素瘤免疫治疗的患者的肿瘤样本进行了基因表达分析。最后,在多个临床前模型中研究了抑制这些靶标对免疫治疗疗效的影响。在这两个互补筛选中,均鉴定出极光激酶是黑色素瘤细胞对 T 细胞介导的细胞毒性耐药的介质。验证了极光激酶抑制剂与体外 T 细胞介导的细胞毒性协同作用。极光激酶抑制介导的对 T 细胞细胞毒性的敏感性部分是由 p21 介导的细胞衰老诱导驱动的。极光激酶和相关蛋白的表达水平与黑色素瘤患者的免疫浸润、对免疫治疗的反应和生存呈负相关。极光激酶抑制与免疫治疗联合在体内的反应不同,表明其活性在肿瘤微环境中的其他因素的影响下发生改变。这些数据表明,极光激酶抑制在体外增强了 T 细胞的细胞毒性,并在某些但不是所有情况下增强了体内的抗肿瘤免疫。需要进一步研究以确定对这种治疗干预的原发性耐药的机制。