State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Sun Yat-sen University, Guangzhou, 510060, P. R. China.
Department of Medical Oncology, Sun Yat-sen University Cancer Center, Guangzhou, 510060, Guangdong, China.
Mol Cancer. 2020 Oct 30;19(1):154. doi: 10.1186/s12943-020-01274-7.
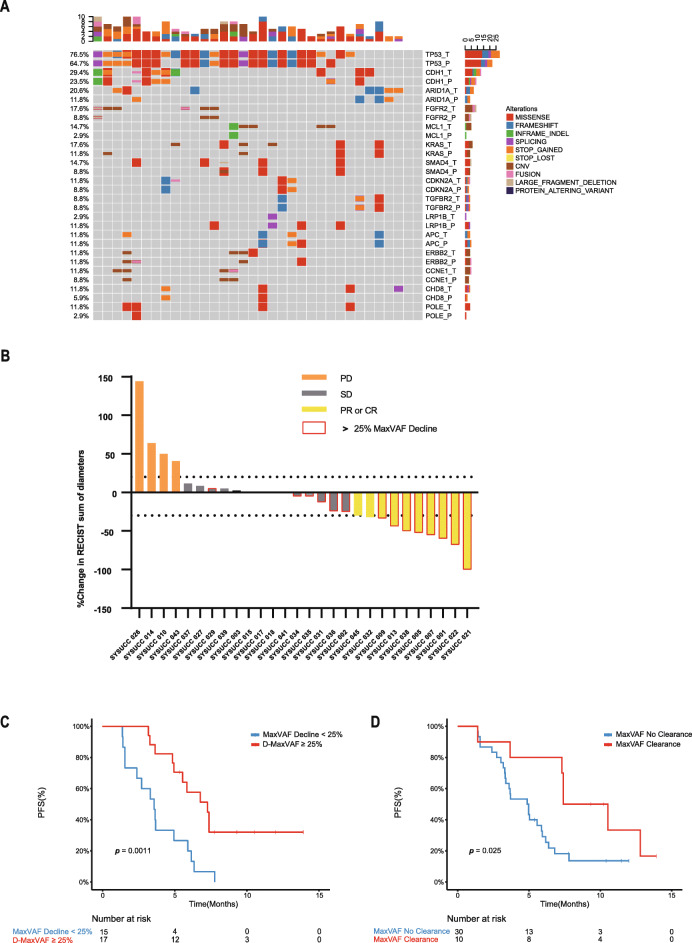
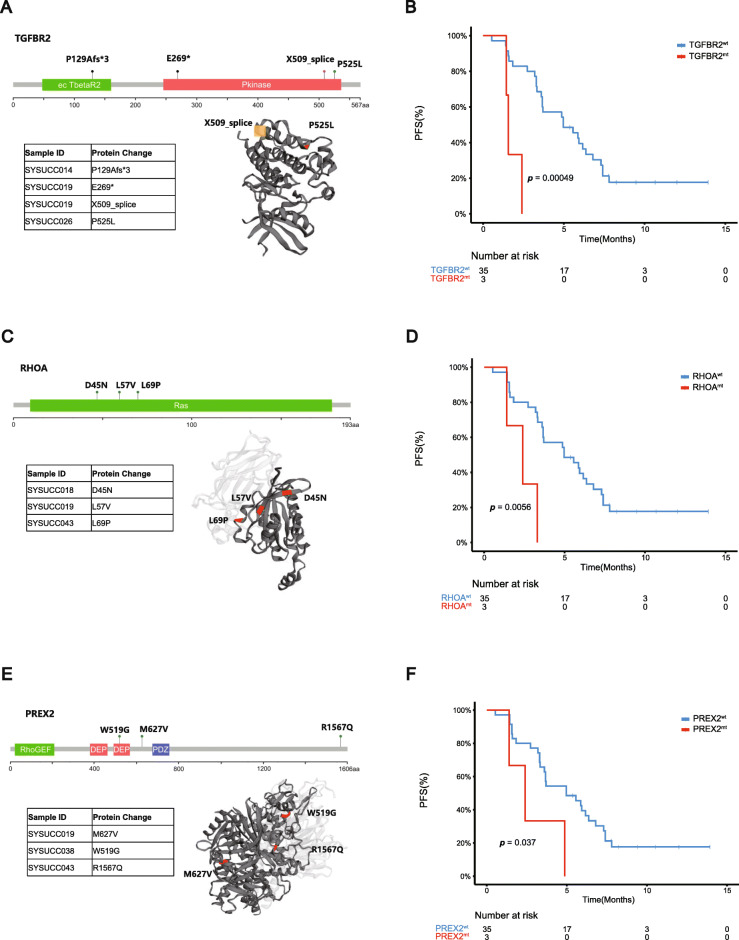
A more common and noninvasive predicting biomarker for programmed cell death 1 (PD-1) antibody remains to be explored. We assessed 46 patients with advanced gastric cancer who received PD-1 antibody immunotherapy and 425-genes next-generation sequencing (NGS) testing. Patients who had a > 25% decline in maximal somatic variant allelic frequency (maxVAF) had a longer progression free survival (PFS) and higher response rate than those who did not (7.3 months vs 3.6 months, p = 0.0011; 53.3% vs 13.3%, p = 0.06). The median PFS of patients with undetectable and detectable post-treatment circulating tumor DNA (ctDNA) was 7.4 months vs. 4.9 months (p = 0.025). Mutation status of TGFBR2, RHOA, and PREX2 in baseline ctDNA influenced the PFS of immunotherapy (p < 0.05). Patients with alterations in CEBPA, FGFR4, MET or KMT2B (p = 0.09) gene had greater likelihood of immune-related adverse events (irAEs). ctDNA can serve as a potential biomarker of the response to immunotherapy in advanced gastric cancers, and its potential role in predicting irAEs worth further exploration.
目前仍需要探索一种更常见且非侵入性的程序性细胞死亡 1(PD-1)抗体预测生物标志物。我们评估了 46 名接受 PD-1 抗体免疫治疗的晚期胃癌患者和 425 基因的下一代测序(NGS)检测。与未达到最大体细胞变异等位基因频率(maxVAF)>25%下降的患者相比,达到该标准的患者具有更长的无进展生存期(PFS)和更高的缓解率(7.3 个月比 3.6 个月,p=0.0011;53.3%比 13.3%,p=0.06)。在治疗后循环肿瘤 DNA(ctDNA)中不可检测和可检测的患者的中位 PFS 分别为 7.4 个月和 4.9 个月(p=0.025)。基线 ctDNA 中 TGFBR2、RHOA 和 PREX2 的突变状态影响免疫治疗的 PFS(p<0.05)。CEBPA、FGFR4、MET 或 KMT2B(p=0.09)基因改变的患者发生免疫相关不良事件(irAEs)的可能性更大。ctDNA 可以作为晚期胃癌对免疫治疗反应的潜在生物标志物,其在预测 irAEs 方面的潜在作用值得进一步探索。