Tougeron David, Louvet Christophe, Desramé Jérôme, Evesque Ludovic, Angelergues Antoine, Carnot Aurélien, Breysacher Gilles, Zaanan Aziz, Etchepare Nicolas, Mabro May, Kaluzinski Laure, Petorin Caroline, Chibaudel Benoist, Aparicio Thomas, Bodere Anaïs, Rinaldi Yves, Le Malicot Karine, Emile Jean-François, Lepage Côme, Baures Aurélia, Djamai Hanane, Taly Valérie, Laurent-Puig Pierre
Department of Gastroenterology and Hepatology, Poitiers University Hospital, Poitiers, France.
Department of Medical Oncology, Institute Mutualiste Montsouris, Paris, France.
Commun Med (Lond). 2025 Apr 24;5(1):136. doi: 10.1038/s43856-025-00867-x.
Efficacy of 2nd line treatment in advanced gastric or gastro-esophageal junction (GEJ) adenocarcinoma remains limited with no identified strong predictor of treatment efficacy. We evaluated the prognostic value of circulating tumor DNA (ctDNA) in predicting the efficacy of immune checkpoint inhibitors (ICI) plus chemotherapy in the randomized PRODIGE 59-FFCD 1707-DURIGAST trial.
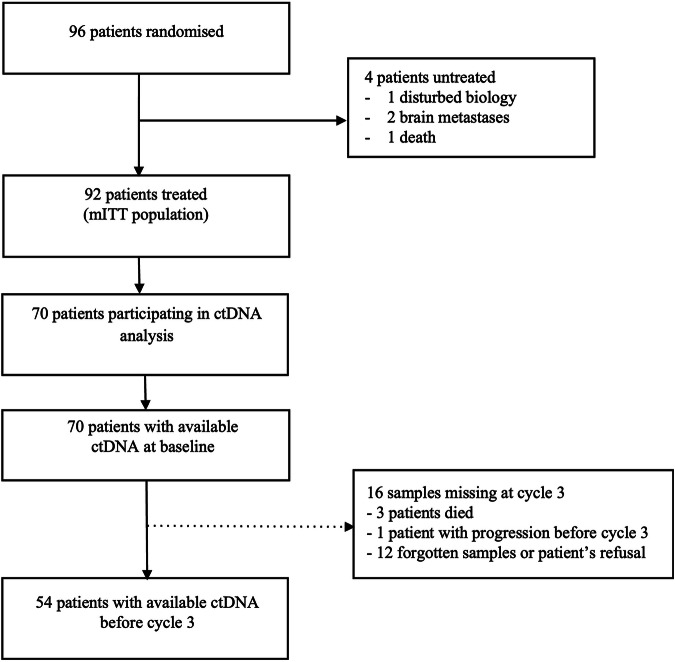
ctDNA was evaluated before treatment (baseline) and at 4 weeks (before the third cycle of treatment, C3) using droplet-digital PCR assays based on the detection of CpG methylation.
Progression-free survival (PFS) and overall survival (OS) were shorter in patients with a high (>1.1 ng/mL) versus low (<1.1 ng/mL) ctDNA concentration at baseline (2.3 vs. 5.8 months; HR = 2.19; 95% CI, 1.09-4.41; p = 0.03 and 4.5 vs. 12.9 months; HR = 2.73; 95% CI, 1.29-5.75; p < 0.01), respectively, after adjustment for identified prognostic variables. Patients with a ctDNA decrease ≤75% between baseline and C3 versus a ctDNA decrease >75% had a worse objective response rate (p = 0.007), shorter PFS (2.2 vs. 7.4 months, HR = 1.90; 95% CI, 1.03-3.51; p = 0.04) and OS (6.6 vs 16.0 months; HR = 2.18; 95% CI, 1.09-4.37; p = 0.03).
An early decrease in ctDNA concentration is a strong predictor of the therapeutic efficacy of ICI plus chemotherapy in advanced gastric/GEJ adenocarcinoma. Clinical Trial Information NCT03959293 (DURIGAST).
晚期胃癌或胃食管交界(GEJ)腺癌二线治疗的疗效仍然有限,尚未确定强有力的疗效预测指标。我们在随机化的PRODIGE 59-FFCD 1707-DURIGAST试验中评估了循环肿瘤DNA(ctDNA)对免疫检查点抑制剂(ICI)联合化疗疗效的预后价值。
在治疗前(基线)和4周时(第三个治疗周期前,即C3),使用基于CpG甲基化检测的液滴数字PCR检测法评估ctDNA。
在对已确定的预后变量进行调整后,基线时ctDNA浓度高(>1.1 ng/mL)的患者与低(<1.1 ng/mL)的患者相比,无进展生存期(PFS)和总生存期(OS)更短(分别为2.3个月对5.8个月;风险比[HR]=2.19;95%置信区间[CI],1.09-4.41;p=0.03)和4.5个月对12.9个月;HR=2.73;95%CI,1.29-5.75;p<0.01)。基线至C3期间ctDNA下降≤75%的患者与ctDNA下降>75%的患者相比,客观缓解率更差(p=0.007),PFS更短(2.2个月对7.4个月,HR=1.90;95%CI,1.03-3.51;p=0.04)和OS更短(6.6个月对16.0个月;HR=2.18;95%CI,1.09-4.37;p=0.03)。
ctDNA浓度的早期下降是晚期胃/GEJ腺癌中ICI联合化疗疗效的强有力预测指标。临床试验信息NCT03959293(DURIGAST)。