The Joseph Sagol Neuroscience Center, Sheba Medical Center, Tel-Hashomer, Israel; Department of Psychiatry, Sheba Medical Center, Tel Hashomer, Israel; Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; Maccabi Healthcare Services, Israel.
Am J Geriatr Psychiatry. 2021 Jan;29(1):1-11. doi: 10.1016/j.jagp.2020.09.022. Epub 2020 Oct 7.
Older adults with type 2 diabetes (T2D) are at increased risk for depression, cognitive decline, and dementia compared to those without T2D. Little is known about the association of simultaneous changes in depression symptoms and cognitive decline over time.
Subjects (n=1021; mean age 71.6 [SD=4.6]; 41.2% female) were initially cognitively normal participants of the Israel Diabetes and Cognitive Decline study who underwent evaluations of depression and cognition approximately every 18 months. Cognitive tests were summarized into four cognitive domains: episodic memory, attention/working memory, executive functions, and semantic categorization. The average of the z-scores of the four domains defined global cognition. Depression symptoms were assessed using the Geriatric Depression Scale, 15-item version. We fit a random coefficients model of changes in depression and in cognitive functions, adjusting for baseline sociodemographic and cardiovascular variables.
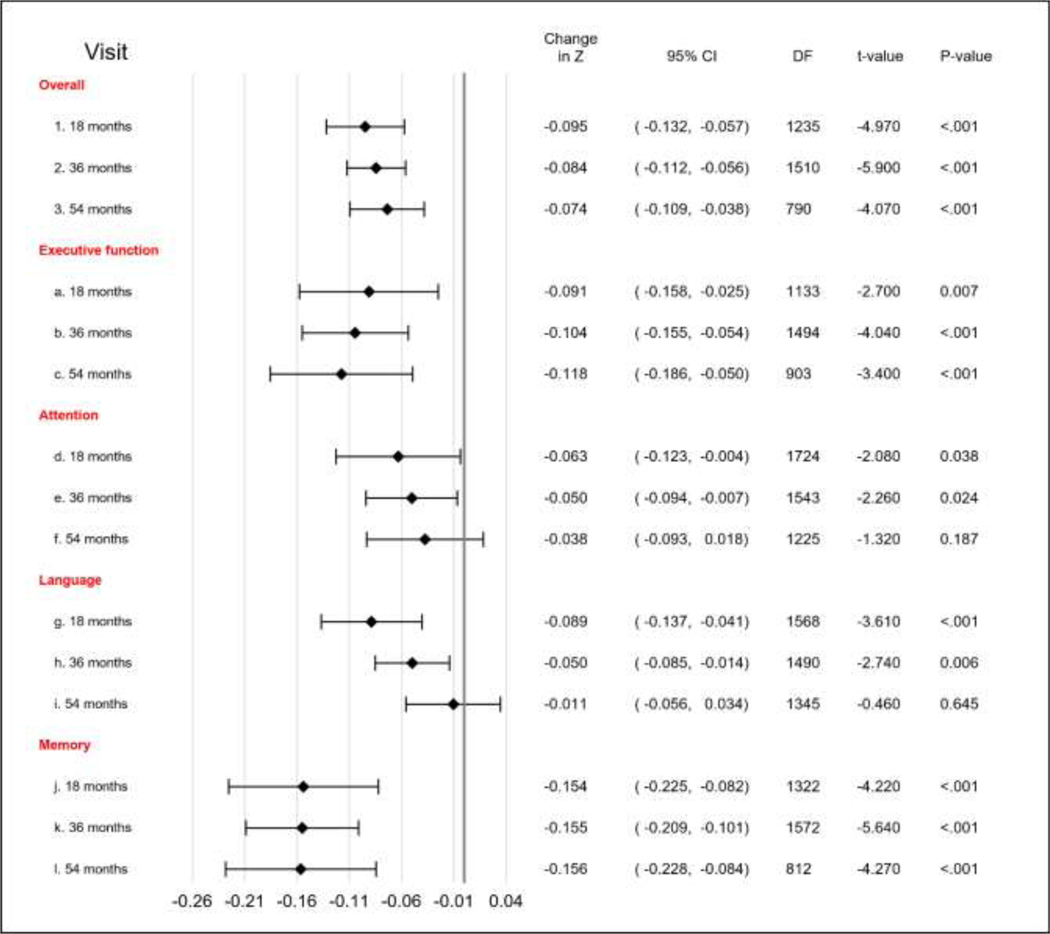
Higher number of depression symptoms at baseline was significantly associated with lower baseline cognitive scores in global cognition (estimate = -0.1175, SE = 0.021, DF = 1,014, t = -5.59; p < 0.001), executive functions (estimate = -0.186, SE = 0.036, DF = 1,013, t = -5.15; p = <0.001), semantic categorization (estimate = -0.155, SE = 0.029, DF = 1,008, t = -5.3; p < 0.001), and episodic memory (estimate = -0.08165, SE = 0.027, DF = 1,035, t = -2.92; p = 0.0036), but not with rate of decline in any cognitive domain. During follow-up, a larger increase in number of depression symptoms, was associated with worse cognitive outcomes in global cognition (estimate = -0.1053, SE = 0.027, DF = 1,612, t = -3.77; p = 0.0002), semantic categorization (estimate = -0.123, SE = 0.036, DF = 1,583, t = -3.36; p = 0.0008), and in episodic memory (estimate = -0.165, SE = 0.055, DF = 1,622, t = -3.02; p = 0.003), but the size of this effect was constant over time.
In elderly with T2D, increase in depression symptoms over time is associated with parallel cognitive decline, indicating that the natural course of the two conditions progresses concurrently and suggesting common underlying mechanisms".
与没有 2 型糖尿病(T2D)的老年人相比,患有 2 型糖尿病的老年人患抑郁症、认知能力下降和痴呆的风险增加。对于抑郁症状随时间同时变化与认知能力下降之间的关联知之甚少。
受试者(n=1021;平均年龄 71.6[SD=4.6];41.2%为女性)最初是以色列糖尿病和认知衰退研究中认知正常的参与者,他们大约每 18 个月接受一次抑郁和认知评估。认知测试被总结为四个认知领域:情景记忆、注意力/工作记忆、执行功能和语义分类。四个领域的 z 分数平均值定义为整体认知。使用老年抑郁量表 15 项版本评估抑郁症状。我们使用随机系数模型来调整基线人口统计学和心血管变量,以评估抑郁和认知功能的变化。
基线时更多的抑郁症状与全球认知(估计值=-0.1175,SE=0.021,DF=1,014,t=-5.59;p<0.001)、执行功能(估计值=-0.186,SE=0.036,DF=1,013,t=-5.15;p<0.001)、语义分类(估计值=-0.155,SE=0.029,DF=1,008,t=-5.3;p<0.001)和情景记忆(估计值=-0.08165,SE=0.027,DF=1,035,t=-2.92;p=0.0036)的基线认知评分显著降低,但与任何认知领域的下降速度无关。在随访期间,抑郁症状数量的较大增加与全球认知(估计值=-0.1053,SE=0.027,DF=1,612,t=-3.77;p=0.0002)、语义分类(估计值=-0.123,SE=0.036,DF=1,583,t=-3.36;p=0.0008)和情景记忆(估计值=-0.165,SE=0.055,DF=1,622,t=-3.02;p=0.003)的认知结果恶化相关,且这种影响的大小在整个过程中是恒定的。
在患有 2 型糖尿病的老年人中,随着时间的推移抑郁症状的增加与认知能力的平行下降有关,这表明这两种情况的自然病程同时进展,并提示存在共同的潜在机制。