Bhatt Parth, Yagnik Priyank J, Saikumar Pavithra, Parmar Narendrasinh, Dave Mihir, Amponsah Jason K, Bhatt Neel S, Sharma Mayank, Thakkar Badal, Donda Keyur, Dapaah-Siakwan Fredrick
Pediatrics, United Hospital Center, Bridgeport, USA.
Pediatrics, University of Kansas School of Medicine-Wichita, Wichita, USA.
Cureus. 2020 Sep 23;12(9):e10611. doi: 10.7759/cureus.10611.
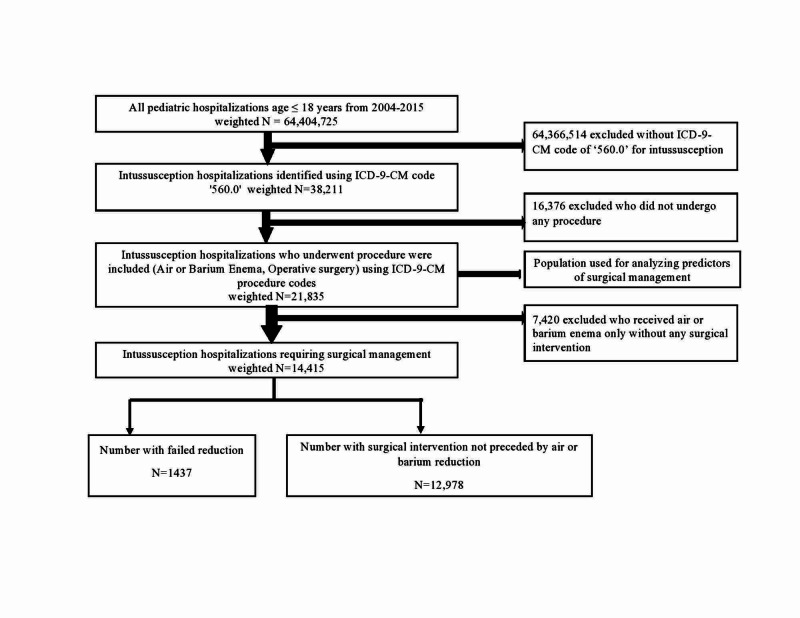
Air or barium enema reduction is becoming increasingly common and safer for pediatric intussusception. However, little is known about trends of pediatric intussusception requiring surgical intervention in the United States. Methods: National Inpatient Sample database was analyzed from 2005-2014 to identify pediatric (≤18 years) intussusceptions along with procedures such as enema and/or surgical intervention. Trends in the rates of surgical intervention were examined according to encounter-level (age, gender, race, comorbidities) and hospital-level (hospital census region, teaching status) characteristics. Outcomes of pediatric intussusception requiring surgical intervention were analyzed in terms of length of stay and cost of hospitalization. Factors associated with surgical intervention were also analyzed. P value of < 0.05 was considered significant. Results: Out of 21,835 intussusception hospitalizations requiring enema or surgical intervention, 14,415 (66%) had surgical intervention; 90% of which (12,978) had no preceding enema. Surgical intervention rates among intussusception hospitalizations varied by age (highest < 1 year), gender (male > females) and race (Hispanics > Whites and Blacks). During the study period, overall surgical intervention rate remained stable (2.2 to 1.7, P=0.07) although it declined in those under 1 year of age. Children with severe disease, gastrointestinal comorbidities over the age of 4 years had increased odds of surgical intervention, whereas hospitalization in large and urban teaching hospitals had decreased odds of surgical intervention. Length of stay and hospital cost remained stable from 2005-2014.
The rates of surgical intervention and resource utilization for pediatric intussusception remained stable from 2005-2014, however they declined significantly in infants. The proportion of intussusception hospitalization requiring surgery remains high and further studies are needed to explore the possible factors.
空气灌肠或钡剂灌肠复位术在小儿肠套叠治疗中越来越常见且更安全。然而,在美国,关于需要手术干预的小儿肠套叠的趋势知之甚少。
分析2005年至2014年的国家住院样本数据库,以确定小儿(≤18岁)肠套叠以及灌肠和/或手术干预等治疗手段。根据患者层面(年龄、性别、种族、合并症)和医院层面(医院所在普查区域、教学状况)的特征,研究手术干预率的趋势。对需要手术干预的小儿肠套叠的住院时长和住院费用等结果进行分析。还分析了与手术干预相关的因素。P值<0.05被视为具有统计学意义。
在21,835例需要灌肠或手术干预的肠套叠住院病例中,14,415例(66%)接受了手术干预;其中90%(12,978例)在手术前未进行灌肠。肠套叠住院病例中的手术干预率因年龄(<1岁最高)、性别(男性>女性)和种族(西班牙裔>白人和黑人)而异。在研究期间,总体手术干预率保持稳定(从2.2降至1.7,P = 0.07),尽管1岁以下儿童的手术干预率有所下降。患有严重疾病、4岁以上有胃肠道合并症的儿童接受手术干预的几率增加,而在大型城市教学医院住院的儿童接受手术干预的几率降低。2005年至2014年,住院时长和住院费用保持稳定。
2005年至2014年,小儿肠套叠的手术干预率和资源利用率保持稳定,但婴儿中的手术干预率显著下降。需要手术治疗的肠套叠住院病例比例仍然很高,需要进一步研究以探索可能的因素。