Wilson Jamie R F, Badhiwala Jetan H, Moghaddamjou Ali, Yee Albert, Wilson Jefferson R, Fehlings Michael G
Nebraska Medical Center, University of Nebraska Medical Center, Omaha, NE 68198, USA.
Spine Program, Department of Surgery, University of Toronto, Toronto, ON M5T 2S8, Canada.
J Clin Med. 2020 Oct 29;9(11):3491. doi: 10.3390/jcm9113491.
The ability of frailty compared to age alone to predict adverse events in the surgical management of Degenerative Cervical Myelopathy (DCM) has not been defined in the literature.
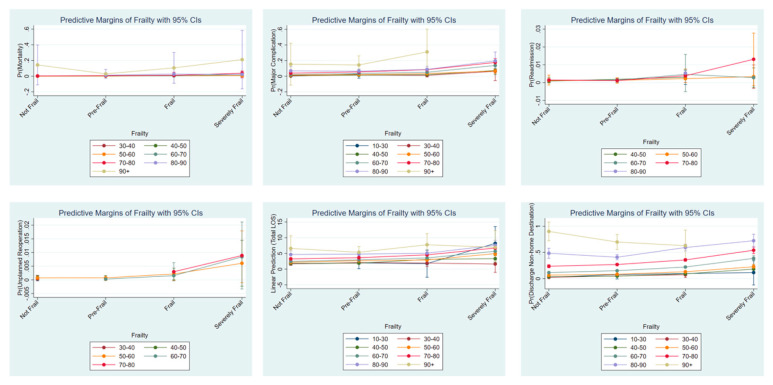
41,369 patients with a diagnosis of DCM undergoing surgery were collected from the National Surgical Quality Improvement Program (NSQIP) Database 2010-2018. Univariate analysis for each measure of frailty (modified frailty index 11- and 5-point; MFI-11, MFI-5), modified Charlson Co-morbidity index and ASA grade) were calculated for the following outcomes: mortality, major complication, unplanned reoperation, unplanned readmission, length of hospital stay, and discharge to a non-home destination. Multivariable modeling of age and frailty with a base model was performed to define the discriminative ability of each measure.
Age and frailty have a significant effect on all outcomes, but the MFI-5 has the largest effect size. Increasing frailty correlated significantly with the risk of perioperative adverse events, longer hospital stay, and risk of a non-home discharge destination. Multivariable modeling incorporating MFI-5 with age and the base model had a robust predictive value (0.85). MFI-5 had a high categorical assessment correlation with a MFI-11 of 0.988 ( < 0.001).
Measures of frailty have a greater effect size and a higher discriminative value to predict adverse events than age alone. MFI-5 categorical assessment is essentially equivalent to the MFI-11 score for DCM patients. A multivariable model using MFI-5 provides an accurate predictive tool that has important clinical applications.
在文献中,与单纯年龄相比,衰弱在预测退行性颈椎病(DCM)手术治疗中的不良事件方面的能力尚未明确。
从2010 - 2018年国家外科质量改进计划(NSQIP)数据库中收集了41369例诊断为DCM并接受手术的患者。对每种衰弱指标(改良衰弱指数11分制和5分制;MFI - 11、MFI - 5)、改良Charlson合并症指数和ASA分级进行单因素分析,以评估以下结局:死亡率、主要并发症、计划外再次手术、计划外再入院、住院时间以及出院至非家庭目的地。对年龄和衰弱进行基于基础模型的多变量建模,以确定每种指标的判别能力。
年龄和衰弱对所有结局均有显著影响,但MFI - 5的效应量最大。衰弱程度增加与围手术期不良事件风险、更长的住院时间以及非家庭出院目的地风险显著相关。将MFI - 5与年龄和基础模型相结合的多变量建模具有强大的预测价值(0.85)。MFI - 5与MFI - 11的分类评估相关性较高,为0.988(<0.001)。
与单纯年龄相比,衰弱指标对预测不良事件具有更大的效应量和更高的判别价值。对于DCM患者,MFI - 5分类评估基本等同于MFI - 11评分。使用MFI - 5的多变量模型提供了一种准确的预测工具,具有重要的临床应用价值。