De Lorenzo Stefania, Tovoli Francesco, Mazzotta Alessandro, Vasuri Francesco, Edeline Julien, Malvi Deborah, Boudjema Karim, Renzulli Matteo, Jeddou Heithem, D'Errico Antonietta, Turlin Bruno, Cescon Matteo, Uguen Thomas, Granito Alessandro, Lièvre Astrid, Brandi Giovanni
Oncologia Medica, Azienda Ospedaliero-Universitaria di Bologna, via Albertoni 15, 40138 Bologna, Italy.
Division of Internal Medicine, Azienda Ospedaliero-Universitaria di Bologna, via Albertoni 15, 40138 Bologna, Italy.
Cancers (Basel). 2020 Oct 29;12(11):3182. doi: 10.3390/cancers12113182.
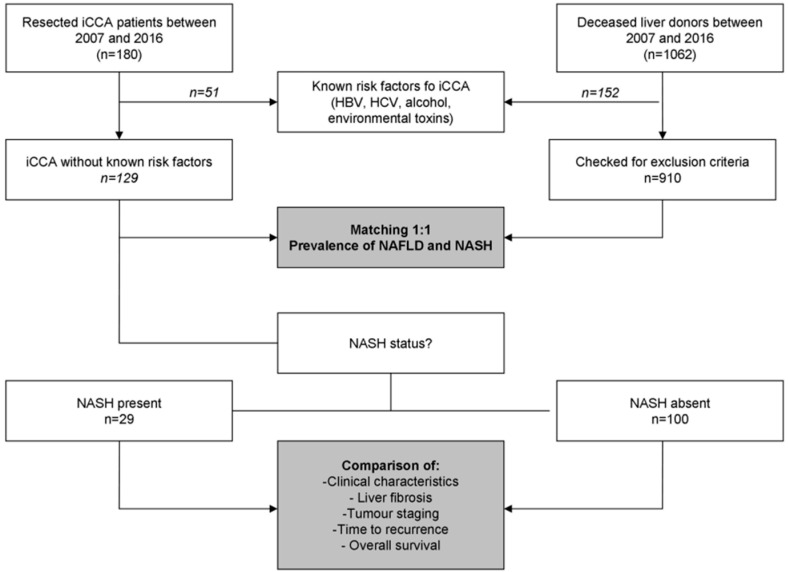
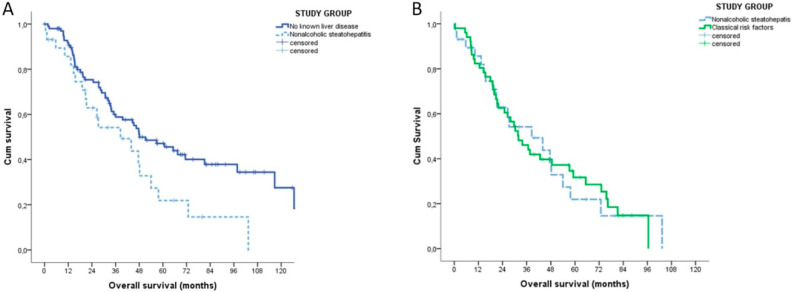
Non-alcoholic fatty liver disease (NAFLD) and its most aggressive form, non-alcoholic steatohepatitis (NASH), are causing a rise in the prevalence of hepatocellular carcinoma. Data about NAFLD/NASH and intrahepatic cholangiocarcinoma (iCCA) are few and contradictory, coming from population registries that do not correctly distinguish between NAFLD and NASH. We evaluated the prevalence of NAFLD and NASH in peritumoral tissue of resected iCCA ( = 180) and in needle biopsies of matched liver donors. Data of iCCA patients were subsequently analysed to compare NASH-related iCCA (Group A), iCCA arisen in a healthy liver (Group B) or in patients with classical iCCA risk factors (Group C). NASH was found in 22.5% of 129 iCCA patients without known risk factors and in 6.2% of matched controls (risk ratio 3.625, 95% confidence interval 1.723-7.626, < 0.001), while NAFLD was equally represented in both groups. The overall survival of NASH-related iCCA was inferior to that of patients with healthy liver (38.5 vs. 48.1 months, = 0.003) and similar to that of patients with known risk factors (31.9 months, = 0.948), regardless of liver fibrosis. The multivariable Cox regression confirmed NASH as a prognostic factor (hazard ratio 1.773, 95% confidence interval 1.156-2.718, = 0.009). We concluded that NASH (but not NAFLD) is a risk factor for iCCA and might affect its prognosis. Dissecting NASH from NAFLD by histology is necessary to correctly assess the actual role of these conditions. Prevention protocols for NASH patients should also consider the risk for iCCA and not only HCC. Mechanistic studies aimed to find a direct pathogenic link between NASH and iCCA could add further relevant information.
非酒精性脂肪性肝病(NAFLD)及其最严重的形式——非酒精性脂肪性肝炎(NASH),正导致肝细胞癌的患病率上升。关于NAFLD/NASH与肝内胆管癌(iCCA)的数据很少且相互矛盾,这些数据来自未能正确区分NAFLD和NASH的人群登记处。我们评估了切除的iCCA瘤周组织(n = 180)以及匹配的肝脏供体针吸活检组织中NAFLD和NASH的患病率。随后对iCCA患者的数据进行分析,以比较NASH相关的iCCA(A组)、发生于健康肝脏的iCCA(B组)或具有经典iCCA危险因素患者的iCCA(C组)。在129例无已知危险因素的iCCA患者中,22.5%发现有NASH,而匹配对照组中这一比例为6.2%(风险比3.625,95%置信区间1.723 - 7.626,P < 0.001),而两组中NAFLD的比例相当。无论肝纤维化情况如何,NASH相关iCCA患者的总生存期均低于肝脏健康患者(38.5个月对48.1个月,P = 0.003),且与具有已知危险因素患者的总生存期相似(31.9个月,P = 0.948)。多变量Cox回归证实NASH是一个预后因素(风险比1.773,95%置信区间1.156 - 2.718,P = 0.009)。我们得出结论,NASH(而非NAFLD)是iCCA的一个危险因素,且可能影响其预后。通过组织学将NASH与NAFLD区分开来,对于正确评估这些情况的实际作用是必要的。NASH患者的预防方案也应考虑iCCA的风险,而不仅仅是肝癌。旨在发现NASH与iCCA之间直接致病联系的机制研究可能会提供更多相关信息。