Dubai Hospital, P. O. Box 7272, Al Baraha, Dubai, UAE.
Dubai Health Authority, Dubai, UAE.
Heart Lung. 2021 Jan-Feb;50(1):1-5. doi: 10.1016/j.hrtlng.2020.10.009. Epub 2020 Oct 20.
Covid-19 has affected 16Millions people worldwide with 644 K death as of July 26th, 2020. It is associated with inflammation and microvascular thrombosis-anticoagulation in widely used in these patients especially in patients with elevated d-Dimers. The significance of anticoagulation in these patients is not yet established. We aim to define the anticoagulation pattern and its impact on outcomes (28-day survival, LOSICU, DVT, and PE and bleeding complications. We also observe if levels of d-Dimers affect the anticoagulation prescription.
We analyzed data of all consecutive patients with Covid-19 ARDS admitted to ICU retrospectively. The primary variable of interest was anticoagulation. The daily dose of anticoagulant medication for each patient was recorded. Survival (28-day survival), Length of stay in ICU (LOSICU), the occurrence of DVT, PE, or bleeding were primary outcome variables. We also recorded confounding factors with potential impact on clinical outcomes. We assign Patients to one of the four groups based on anticoagulant dosing during the ICU (increasing dose, decreasing dose, increase followed by a decrease, multiple changes). We analyze the effect of different anticoagulation dosing strategies on 28-day survival, LOSICU, the occurrence of DVT, PE, and bleeding. We also observe if levels of d-Dimers affect the anticoagulation prescription.
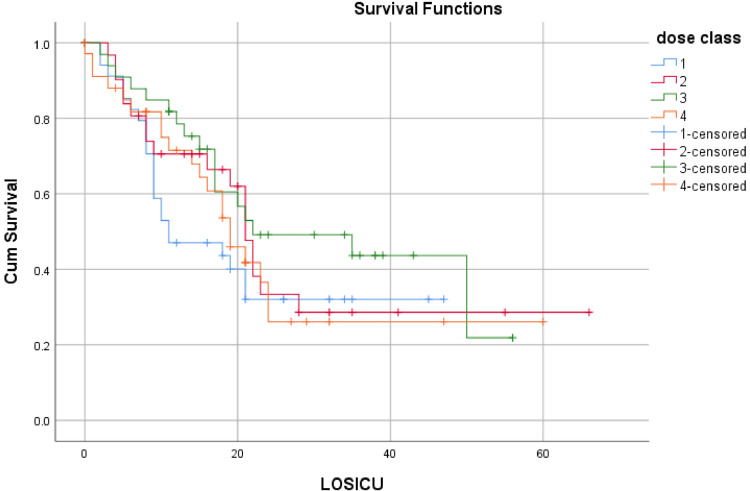
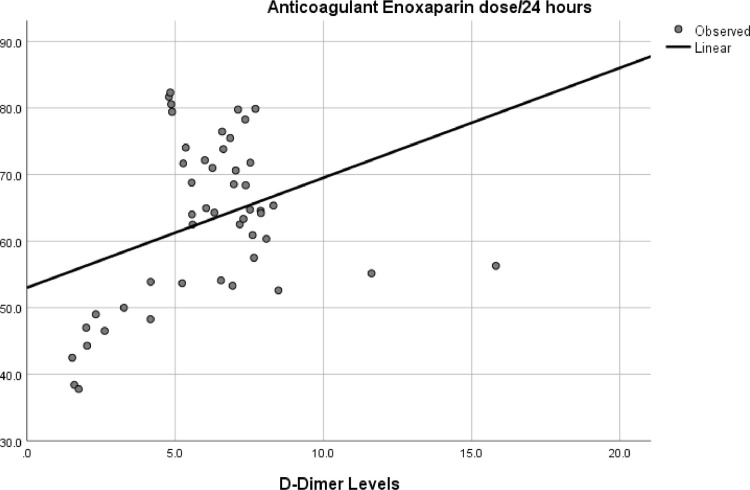
The sample includes 149 patients. The most frequently used medication was subcutaneous Enoxaparin (85.2%). The Enoxaparin mean dose per day for the whole sample was 49.5 mg + 15.7 (mean + SD). There was no significant difference in doses of anticoagulants between survivors and nonsurvivors (62.8 mg + 21.7 mg vs. 61.2 mg + 25.7 mg, p 0.3). Multinomial regression showed no difference in 28-day survival among four-dose modification (increasing dose, decreasing dose, increase followed by a decrease, multiple changes). Logistic regression showed that BMI, d-Dimers, platelets, and the use of mechanical ventilation predict 28-day survival. Kaplan-Meier Survival plots for 4 anticoagulant groups showed no survival advantage for any anticoagulant strategy. Secondary outcome analysis showed that d-dimer levels significantly affect anticoagulants doses.
Prescription of anticoagulation is quite variable in patients admitted to ICU for Covid-19 associated ARDS. Anticoagulation dosing strategy has no significant effect on 28-day survival, LOSICU, the occurrence of DVT, PE, or bleeding.
本研究旨在明确 COVID-19 相关 ARDS 患者的抗凝模式及其对预后(28 天生存率、住 ICU 时间、DVT、PE 和出血并发症)的影响,并观察 d-二聚体水平是否影响抗凝药物的使用剂量。
我们回顾性分析了因 COVID-19 所致 ARDS 而入住 ICU 的所有连续患者的数据。主要观察变量为抗凝治疗。记录每位患者的抗凝药物日剂量。28 天生存率、住 ICU 时间、DVT、PE 和出血并发症是主要的观察终点。我们还记录了可能影响临床结局的混杂因素。根据 ICU 期间抗凝药物的使用剂量,将患者分为以下 4 组:剂量递增、剂量递减、先增后减、多次调整。分析不同抗凝药物剂量策略对 28 天生存率、住 ICU 时间、DVT、PE 和出血并发症的影响,并观察 d-二聚体水平是否影响抗凝药物的使用剂量。
共纳入 149 例患者,最常使用的药物为皮下依诺肝素(85.2%)。全样本依诺肝素的平均日剂量为 49.5mg+15.7(均值+标准差)。幸存者和非幸存者的抗凝药物剂量无显著差异(62.8mg+21.7mg 比 61.2mg+25.7mg,p=0.3)。多分类回归分析显示,4 种剂量调整方案(剂量递增、剂量递减、先增后减、多次调整)对 28 天生存率无影响。Logistic 回归分析显示 BMI、d-二聚体、血小板和机械通气与 28 天生存率相关。Kaplan-Meier 生存曲线显示,4 种抗凝药物治疗组间无生存优势。次要结局分析显示,d-二聚体水平显著影响抗凝药物剂量。
COVID-19 相关 ARDS 患者的抗凝治疗方案差异较大。抗凝药物剂量策略对 28 天生存率、住 ICU 时间、DVT、PE 和出血并发症无显著影响。