Caviglia Gian Paolo, Ciruolo Michela, Abate Maria Lorena, Carucci Patrizia, Rolle Emanuela, Rosso Chiara, Olivero Antonella, Troshina Giulia, Risso Alessandra, Nicolosi Aurora, Ribaldone Davide Giuseppe, Armandi Angelo, Tandoi Francesco, Saracco Giorgio Maria, Bugianesi Elisabetta, Ciancio Alessia, Gaia Silvia
Department of Medical Sciences, University of Turin, 10100 Turin, Italy.
Division of Gastroenterology, Città della Salute e della Scienza University-Hospital, 10100 Turin, Italy.
Cancers (Basel). 2020 Oct 31;12(11):3218. doi: 10.3390/cancers12113218.
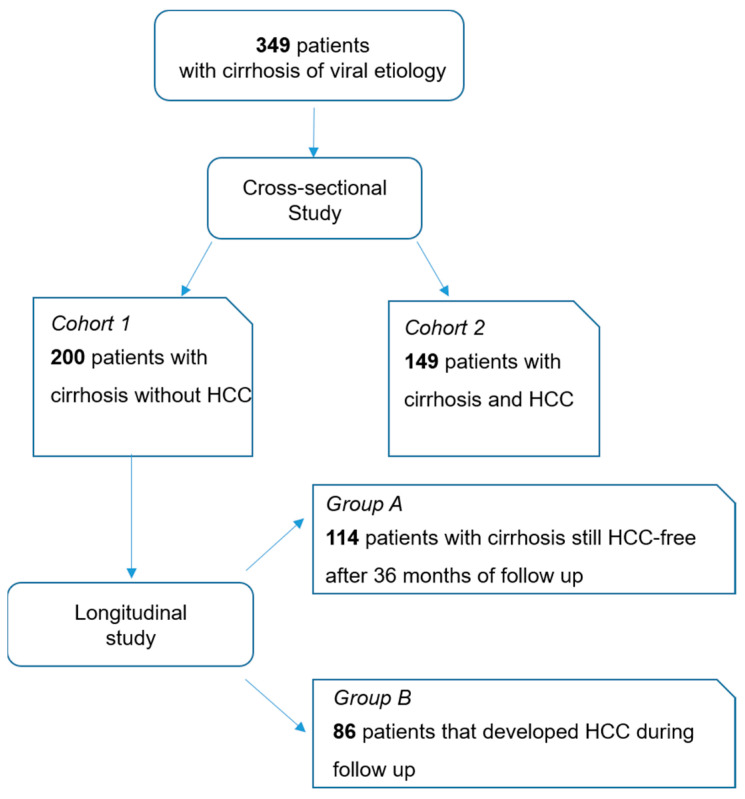
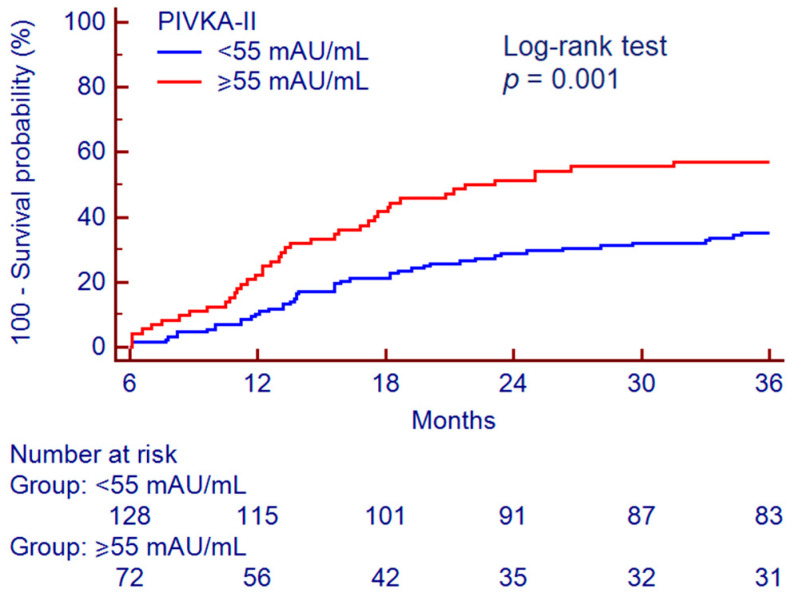
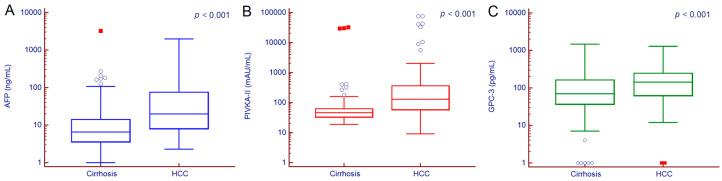
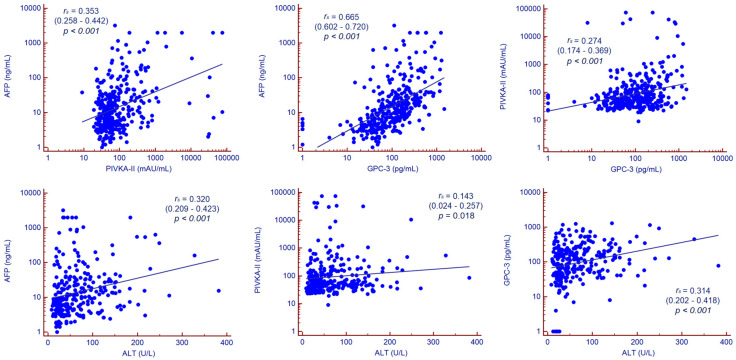
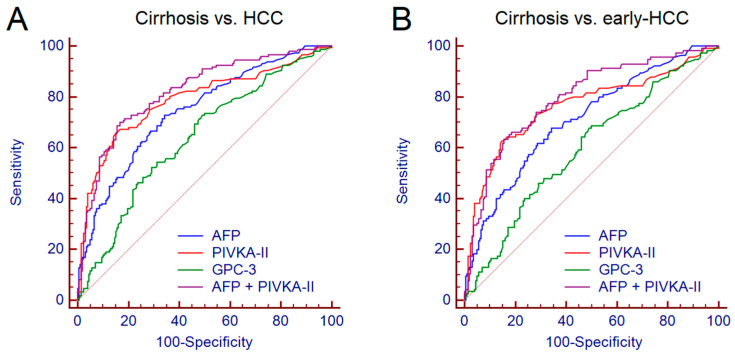
International guidelines recommend the use of ultrasound as a surveillance tool for hepatocellular carcinoma (HCC) in patients with cirrhosis, while the role of serum biomarkers is still debated. We investigated serum alpha-fetoprotein (AFP), protein induced by vitamin K absence or antagonist II (PIVKA-II) and glypican-3 (GPC-3) diagnostic accuracy for HCC detection and prediction in patients with liver cirrhosis of viral etiology under surveillance. A total of 349 patients (200 cirrhosis and 149 HCC) were enrolled. The 200 patients with cirrhosis consisted of 114 patients still HCC-free after 36 months of follow-up and 86 patients that developed HCC after 13.8 (11.0-19.8) months. AFP, PIVKA-II and GPC-3 were measured in serum samples collected at tumor diagnosis in the 149 patients with HCC, and at the beginning of follow-up in the 200 patients with cirrhosis. The higher performance for HCC detection was observed for PIVKA-II (area under the curve (AUC) = 0.790), followed by AFP (AUC = 0.737) and GPC-3 (AUC = 0.637); the combination of AFP + PIVKA-II improved the diagnostic accuracy to AUC = 0.822. Serum PIVKA-II values, but not AFP and GPC-3, were significantly higher in the 86 cirrhotics that developed HCC compared with the 114 cirrhotics still HCC-free after 36 months of follow-up ( = 0.020). PIVKA-II ≥ 55 mAU/mL allowed to identify patients with cirrhosis at higher risk of HCC development (Log-rank test, < 0.001; adjusted Hazard Ratio = 1.99, = 0.001). In conclusion, the measurement of PIVKA-II in patients with cirrhosis may be useful to tailor personalized surveillance strategies.
国际指南推荐将超声作为肝硬化患者肝细胞癌(HCC)的监测工具,而血清生物标志物的作用仍存在争议。我们研究了血清甲胎蛋白(AFP)、维生素K缺乏或拮抗剂II诱导蛋白(PIVKA-II)和磷脂酰肌醇蛋白聚糖-3(GPC-3)在监测下的病毒性病因肝硬化患者中检测和预测HCC的诊断准确性。共纳入349例患者(200例肝硬化患者和149例HCC患者)。200例肝硬化患者中,114例在随访36个月后仍未发生HCC,86例在13.8(11.0-19.8)个月后发生HCC。在149例HCC患者的肿瘤诊断时以及200例肝硬化患者的随访开始时采集血清样本,检测AFP、PIVKA-II和GPC-3。PIVKA-II检测HCC的性能更高(曲线下面积(AUC)=0.790),其次是AFP(AUC=0.737)和GPC-3(AUC=0.637);AFP+PIVKA-II联合使用可将诊断准确性提高到AUC=0.822。与随访36个月后仍未发生HCC的114例肝硬化患者相比,86例发生HCC的肝硬化患者的血清PIVKA-II值显著更高(P=0.020),而AFP和GPC-3则无显著差异。PIVKA-II≥55 mAU/mL可识别肝硬化患者中HCC发生风险较高的患者(对数秩检验,P<0.001;调整后风险比=1.99,P=0.001)。总之,检测肝硬化患者的PIVKA-II可能有助于制定个性化的监测策略。