Kalidindi Kalyan Kumar Varma, Sath Sulaiman
Indian Spinal Injuries Center, New Delhi, India.
Asian J Neurosurg. 2020 Aug 28;15(3):756-758. doi: 10.4103/ajns.AJNS_240_20. eCollection 2020 Jul-Sep.
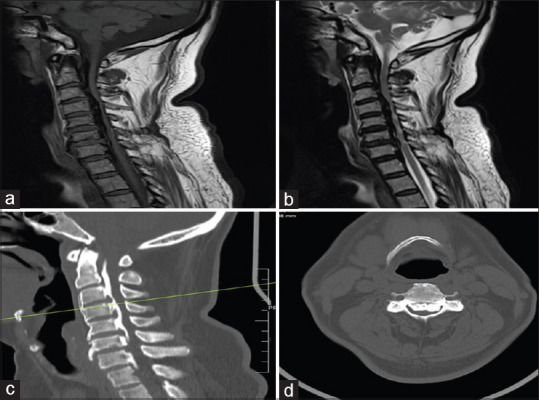
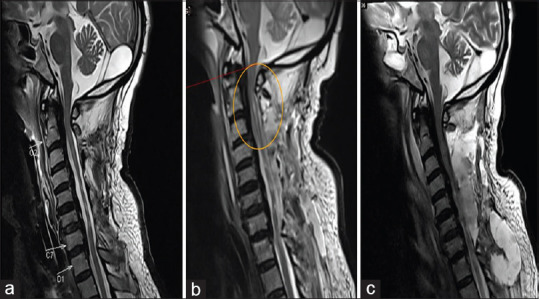
White cord syndrome (WCS) is a rare case of severe neurological deterioration after surgical decompression for cervical myelopathy. It was proposed to be secondary to an ischemia/reperfusion injury. An association of WCS with a hypoxic brain injury (HBI) has not been documented. A 63-year-old man presented to us with progressive symptoms of cervical myelopathy. Computed tomography scan and magnetic resonance imaging (MRI) scan findings were suggestive of an ossified posterior longitudinal ligament with cord atrophy and myelomalacia changes. He was managed surgically by decompression and fusion through a posterior approach. During the surgery, there was a sudden loss of neuromonitoring signals after laminectomy, and wake-up assessment revealed neurological deterioration. Immediate postoperative imaging revealed adequately placed screws and adequate cord decompression. A high dose of intravenous steroids was given. Repeat MRI scan on the 3 postoperative day suggested cord edema over a large area on T2-weighted images. He was diagnosed as WCS and managed conservatively. He had persistent abdominal distension postoperatively, and a diagnostic endoscopy was advised. At the start of the procedure, the patient had a sudden-onset loss of consciousness. Electrocardiogram suggested bradyarrhythmias with hypotension. The patient was resuscitated, intubated, and shifted to intensive care unit. He was diagnosed to have a HBI. He was managed with multidisciplinary rehabilitation and discharged at 4 months' postoperatively with stable vitals. There was no improvement in the neurology or his consciousness. Spine surgeons have to be aware of this potentially disastrous complication of WCS. One should take adequate postoperative care to avoid preventable complications like HBI associated with it.
白脊髓综合征(WCS)是颈椎脊髓病手术减压后严重神经功能恶化的罕见病例。它被认为继发于缺血/再灌注损伤。WCS与缺氧性脑损伤(HBI)的关联尚未见文献记载。一名63岁男性因颈椎脊髓病的进行性症状前来就诊。计算机断层扫描和磁共振成像(MRI)扫描结果提示后纵韧带骨化伴脊髓萎缩和脊髓软化改变。他接受了后路减压融合手术治疗。手术过程中,椎板切除术后神经监测信号突然消失,唤醒评估显示神经功能恶化。术后即刻影像学检查显示螺钉位置合适,脊髓减压充分。给予大剂量静脉类固醇治疗。术后第3天重复MRI扫描显示T2加权图像上大面积脊髓水肿。他被诊断为WCS并接受保守治疗。他术后持续腹胀,建议进行诊断性内镜检查。在检查开始时,患者突然意识丧失。心电图提示缓慢性心律失常伴低血压。患者接受复苏、插管,并转入重症监护病房。他被诊断为患有HBI。他接受了多学科康复治疗,术后4个月生命体征稳定出院。神经功能或意识无改善。脊柱外科医生必须意识到WCS这种潜在的灾难性并发症。应采取充分的术后护理措施,以避免与之相关的如HBI等可预防并发症。