Department of Global Health and Development, Faculty of Public Health & Policy, London School of Hygiene and Tropical Medicine, London, UK
Department of Immunisation, Hepatitis and Blood Safety, Public Health England, London, UK.
BMJ Open. 2020 Nov 3;10(11):e038963. doi: 10.1136/bmjopen-2020-038963.
To evaluate the usability and acceptability of an electronic consent pilot intervention for school-based immunisations and assess its impact on consent form returns and human papilloma virus (HPV) vaccine uptake.
Mixed-methods theory-informed study applying qualitative methods to examine the usability and acceptability of the intervention and quantitative methods to assess its impact.
The intervention was piloted in 14 secondary schools in seven London boroughs in 2018. Intervention schools were matched with schools using paper consent based on the proportion of students with English as a second language and students receiving free school meals. Participants included nurses, data managers, school-link staff, parents and adolescents.
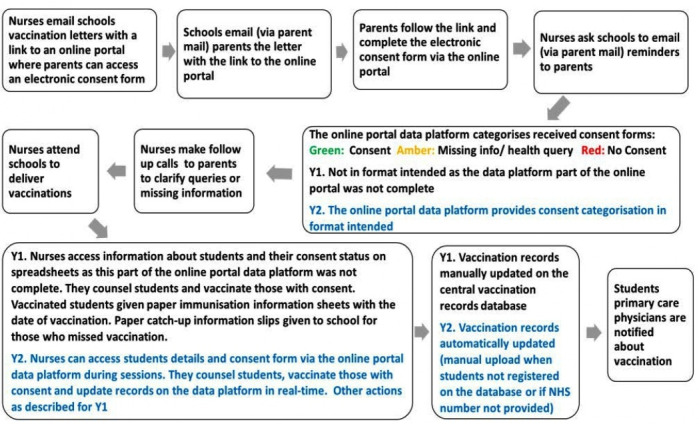
An electronic consent portal where parents could record whether they agreed to or declined vaccination, and nurses could access data to help them manage the immunisation programme.
Comparison of consent form return rates and HPV vaccine uptake between intervention and matched schools.
HPV vaccination uptake did not differ between intervention and matched schools, but timely consent form return was significantly lower in intervention schools (73.3% vs 91.6%, p=0.008). The transition to using electronic consent was not straightforward, while schools and staff understood the potential benefits, they found it difficult to adapt to new ways of working which removed some level of control from schools. Reasons for lower consent form return in e-consent schools included difficulties encountered by some parents in accessing and using the intervention. Adolescents highlighted the potential for electronic consent to by-pass their information needs.
The pilot intervention did not improve consent form return or vaccine uptake due to challenges encountered in transitioning to new working practice. New technologies require embedding before they become incorporated in everyday practice. A re-evaluation once stakeholders are accustomed with electronic consent may be required to understand its impact.
评估基于学校免疫接种的电子知情同意书试点干预措施的可用性和可接受性,并评估其对知情同意书返回率和人乳头瘤病毒(HPV)疫苗接种率的影响。
混合方法理论指导研究,应用定性方法检查干预措施的可用性和可接受性,应用定量方法评估其影响。
该干预措施于 2018 年在伦敦 7 个行政区的 14 所中学进行试点。干预学校与使用纸质知情同意书的学校进行匹配,匹配依据是英语为第二语言的学生比例和获得免费校餐的学生比例。参与者包括护士、数据管理员、学校联络人员、家长和青少年。
电子知情同意门户,家长可以在此处记录他们是否同意或拒绝接种疫苗,护士可以访问数据以帮助他们管理免疫接种计划。
干预组和匹配组学校的知情同意书返回率和 HPV 疫苗接种率比较。
HPV 疫苗接种率在干预组和匹配组学校之间没有差异,但干预组学校及时返回知情同意书的比例明显较低(73.3%比 91.6%,p=0.008)。向电子知情同意过渡并不简单,尽管学校和工作人员理解潜在的好处,但他们发现很难适应新的工作方式,这使学校失去了一定程度的控制。电子知情同意学校知情同意书返回率较低的原因包括一些家长在访问和使用干预措施时遇到困难。青少年强调电子知情同意可能绕过他们的信息需求。
由于在向新工作方式过渡中遇到的挑战,试点干预措施并未提高知情同意书返回率或疫苗接种率。新技术需要在融入日常实践之前进行嵌入。一旦利益相关者习惯了电子知情同意,可能需要重新评估以了解其影响。