Lambertini Matteo, Agbor-Tarh Dominique, Metzger-Filho Otto, Ponde Noam F, Poggio Francesca, Hilbers Florentine S, Korde Larissa A, Chumsri Saranya, Werner Olena, Del Mastro Lucia, Caparica Rafael, Moebus Volker, Moreno-Aspitia Alvaro, Piccart Martine J, de Azambuja Evandro
Department of Internal Medicine and Medical Specialties (DiMI), School of Medicine, University of Genova, Genova, Italy; Department of Medical Oncology, U.O.C Clinica di Oncologia Medica, IRCCS Ospedale Policlinico San Martino, Genova, Italy.
Frontier Science Scotland, Kingussie, UK.
ESMO Open. 2020 Nov;5(6):e000979. doi: 10.1136/esmoopen-2020-000979.
In HER2-positive breast cancer, time elapsed between completion of (neo)adjuvant trastuzumab and diagnosis of metastatic disease ('trastuzumab-free interval', TFI) is crucial to choose the optimal first-line treatment. Nevertheless, there is no clear evidence to support its possible prognostic role.
In the Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation (ALTTO) trial, patients with HER2-positive early breast cancer were randomised to 1 year of either trastuzumab alone, lapatinib alone, their sequence or their combination. This exploratory analysis included only patients in the trastuzumab alone or trastuzumab plus lapatinib arms who developed a distant disease-free survival (DDFS) event. Overall survival (OS) was defined as time between date of DDFS event and death; age at diagnosis, tumour size and hormone receptor status were the variables included in the multivariate models.
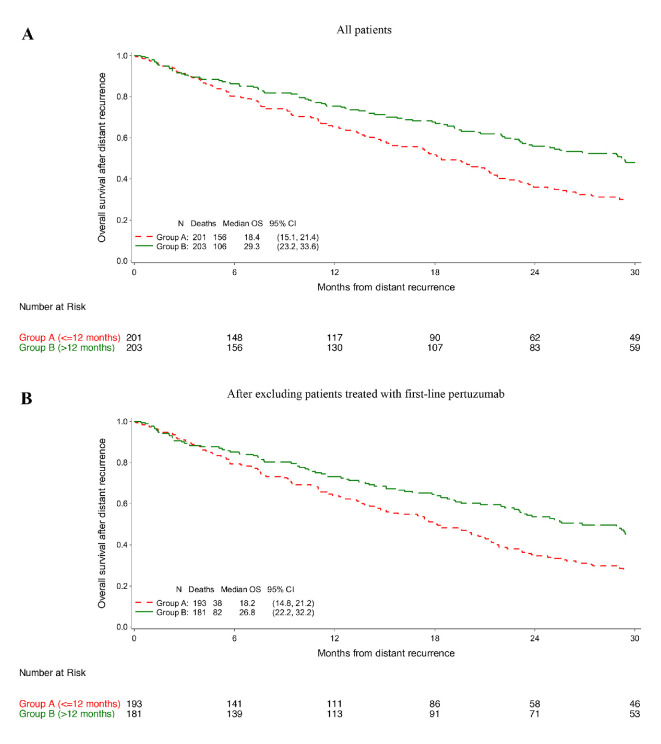
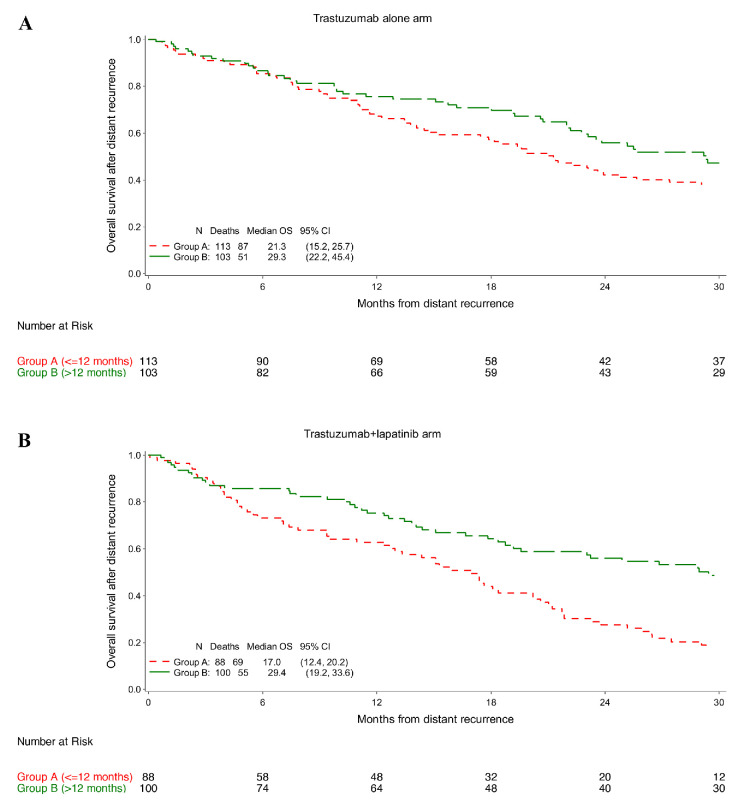
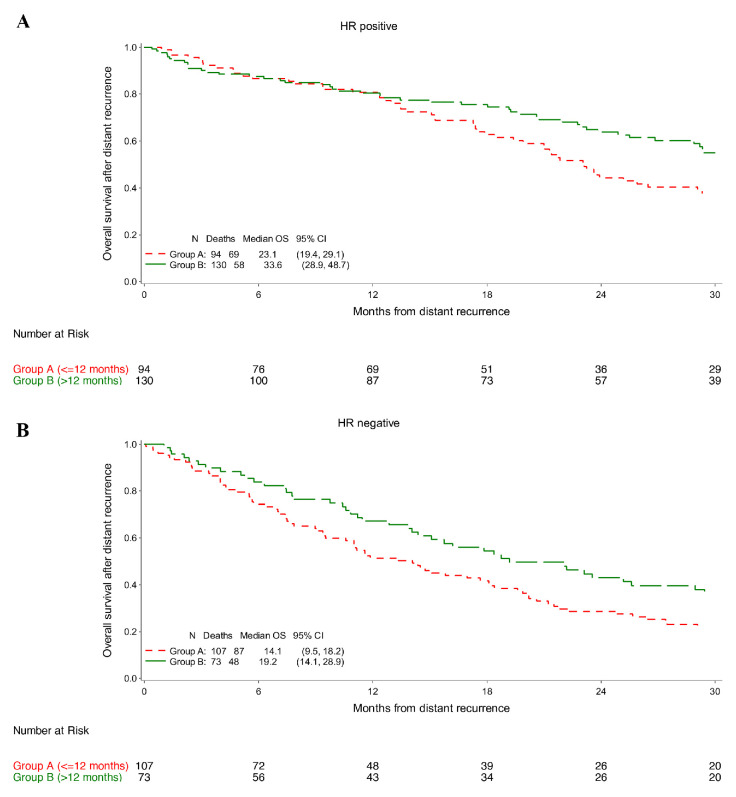
Out of 8381 patients included in ALTTO, 404 patients in the trastuzumab alone and trastuzumab plus lapatinib arms developed a DDFS event, of which 201 occurred 12 months (group A) and 203 >12 months (group B) after completion of adjuvant trastuzumab. No significant difference in location of first DDFS event was observed (p=0.073); a numerically higher number of patients in group A than in group B developed brain metastasis (26% vs 15%). Choice of first-line therapy differed between the two groups (p=0.022): in group A, more patients received lapatinib (25% vs 11%) and less pertuzumab (8% vs 17%). Median OS was 29.3 and 18.4 months in groups B and A, respectively (adjusted HR 0.69; 95% CI 0.54-0.89; p=0.004). The longer OS for patients in group B was observed across the analysed subgroups without interaction according to hormone receptor status (p=0.814) nor type of administered adjuvant anti-HER2 treatment (p=0.233).
TFI has prognostic value in patients with HER2-positive early breast cancer treated with adjuvant trastuzumab-based therapy. TFI is a valid tool to better individualise clinical recommendations and to design future first-line treatment trials for metastatic patients.
在人表皮生长因子受体2(HER2)阳性乳腺癌中,(新)辅助曲妥珠单抗治疗结束至转移性疾病诊断之间的时间间隔(“无曲妥珠单抗间期”,TFI)对于选择最佳一线治疗至关重要。然而,尚无明确证据支持其可能的预后作用。
在辅助性拉帕替尼和/或曲妥珠单抗治疗优化(ALTTO)试验中,HER2阳性早期乳腺癌患者被随机分为接受1年单药曲妥珠单抗、单药拉帕替尼、二者序贯或联合治疗。这项探索性分析仅纳入了单药曲妥珠单抗组或曲妥珠单抗联合拉帕替尼组中发生远处无病生存(DDFS)事件的患者。总生存期(OS)定义为DDFS事件日期至死亡的时间;诊断时年龄、肿瘤大小和激素受体状态是多变量模型中的变量。
在ALTTO纳入的8381例患者中,单药曲妥珠单抗组和曲妥珠单抗联合拉帕替尼组有404例患者发生DDFS事件,其中201例在辅助曲妥珠单抗治疗结束后12个月内发生(A组),203例在12个月后发生(B组)。首次DDFS事件的发生部位无显著差异(p = 0.073);A组发生脑转移的患者数量在数值上高于B组(26%对15%)。两组的一线治疗选择不同(p = 0.022):在A组,更多患者接受拉帕替尼治疗(25%对11%),接受帕妥珠单抗治疗的患者较少(8%对17%)。B组和A组的中位OS分别为29.3个月和18.4个月(校正风险比0.69;95%置信区间0.54 - 0.89;p = 0.004)。在根据激素受体状态(p = 0.814)和辅助抗HER2治疗类型(p = 0.233)进行分析的亚组中,均观察到B组患者的OS更长,且无相互作用。
TFI对接受基于曲妥珠单抗的辅助治疗的HER2阳性早期乳腺癌患者具有预后价值。TFI是一种有效的工具,可更好地实现临床建议个体化,并为转移性患者设计未来的一线治疗试验。